Revista Biomédica Revisada Por Pares

 Para Descargar PDF debe Abrir sesión.
Para Descargar PDF debe Abrir sesión.
Palabras clave: aqueous shunt, trabeculectomy, Epistemonikos, GRADE.
INTRODUCTION
Aqueous shunt has emerged as an alternative technique to trabeculectomy, which is considered the standard treatment for glaucoma surgery. Currently, it is mainly indicated after failure of trabeculectomy or in some types of glaucoma with high risk of failure. However, there is still controversy regarding its effectiveness compared to trabeculectomy.
METHODS
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS
We identified five systematic reviews including nine studies overall, of which four were randomized trials. We concluded that aqueous shunt might increase the qualified success compared to trabeculectomy, but it is not clear whether it has any effect on the rest of the critical outcomes for decision-making because the certainty of the evidence is very low.
According to the World Health Organization, glaucoma is the second cause of blindness worldwide. Among the risk factors for its development, intraocular pressure (IOP) is the only one that can be modified.
Since the end of the last century, the introduction of aqueous shunt has emerged as an alternative surgery to trabeculectomy. The aqueous shunt can be defined as a silicone tube with a lumen attached to an explant plate. Currently, its main indication is for glaucoma with failed trabeculectomy or in some types of glaucoma with a high risk of failure (for example, neovascular or uveitic glaucoma). Over the years, the use of aqueous shunt has spread, being currently chosen as primary surgery by many specialists. However, there is controversy about this last scenario.
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
|
What is the evidence. |
We found five systematic reviews [1], [2], [3], [4], [5] including nine primary studies reported in 16 references [6], [7], [8], [9], [10], [11], [12], [13], [14], [15], [16], [17], [18], [19], [20], [21], of which four correspond to randomized controlled trials, reported in 11 references [7], [8], [9], [10], [11], [12], [13], [16], [17], [20], [21]. However, one trial [16] was performed in pediatric population with aphakic glaucoma, which is not considered comparable with the rest of patients, so it was excluded from this analysis. This table and the summary in general are based on three randomized trials [10], [20], [21], since the inclusion of the observational studies did not increase the certainty of the evidence or added additional information. |
|
What types of patients were included* |
All trials included patients with glaucoma, with an average age of 53.9 years, of both genders, with average IOP of 25.96 mmHg (25.46 mmHg in the aqueous shunt arm, and 26.45 mmHg in the trabeculectomy arm). Regarding the type of glaucoma, one trial included patients with primary open-angle glaucoma, chronic angle-closure glaucoma, pseudoexfoliative glaucoma, pigmentary glaucoma [10], one trial included patients with primary open-angle glaucoma, primary angle-closure glaucoma, neovascular glaucoma, uveitic glaucoma and traumatic glaucoma [20] and one trial included primary open-angle glaucoma and angle-closure glaucoma [21]. In terms of the severity of glaucoma, all trials included patients with indication for surgical treatment [10], [20], [21]. One trial included patients both refractory to medical management and to surgical management (previous trabeculectomy, cataract extraction surgery, or both) [10]. One trial included patients refractory to medical management, and a proportion of patients refractory to surgical management (29.0% in the aqueous shunt arm, 43.6% in the trabeculectomy arm, without specifying the type of previous surgical intervention) [20]. One trial included only patients refractory to medical treatment, excluding patients with previous intraocular surgery [21]. |
|
What types of interventions were included* |
All trials compared aqueous shunt with trabeculectomy [10], [20], [21]. |
|
What types of outcomes |
The trials evaluated multiple outcomes, which were grouped by the systematic reviews as follows:
The average follow-up of the trials was 40 months, with a range between 12 and 60 months. |
* The information about primary studies is extracted from the systematic reviews identified, unless otherwise specified.
The information about the effects of the use of aqueous shunts compared to trabeculectomy is based on three randomized trials involving 452 eyes [10], [20], [21].
All trials reported the mean intraocular pressure at the end of follow-up (320 eyes), change in visual acuity at one year (360 eyes), need of reintervention (452 eyes) and narrow anterior chamber (452 eyes) [10], [20], [21]. Two trials evaluated choroidal effusion (329 eyes) [10], [20]. Only one trial evaluated complete success at the end of follow-up (157 eyes), qualified success at the end of follow-up (157 eyes) and persistent corneal edema (212 eyes) [10].
The summary of findings is as follows:
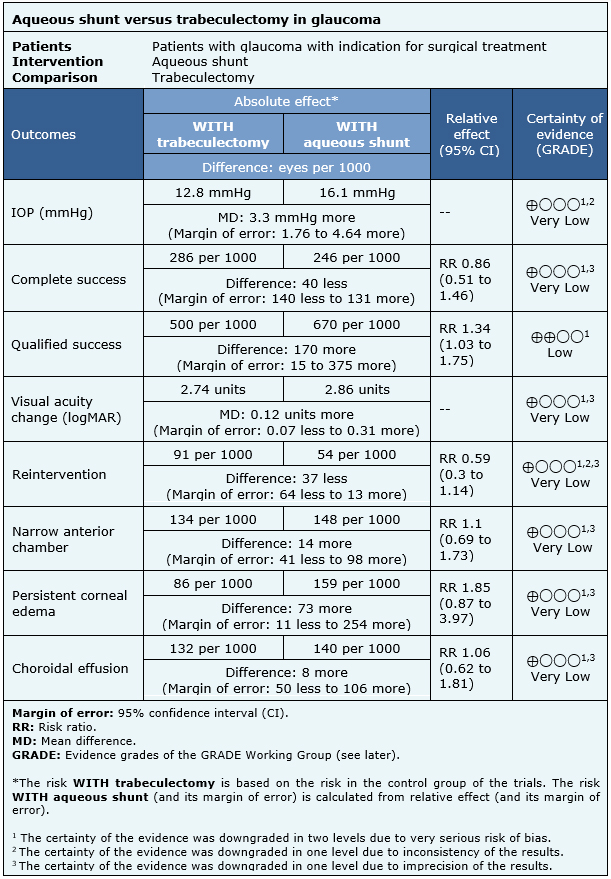
| Follow the link to access the interactive version of this table (Interactive Summary of Findings – iSoF) |

|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
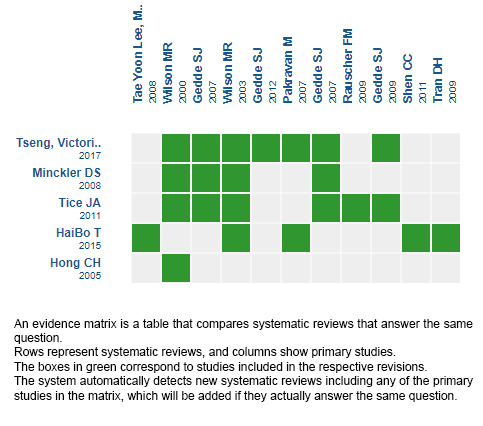
Follow the link to access the interactive version: Aqueous shunt versus trabeculectomy for glaucoma
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
 Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
INTRODUCTION
Aqueous shunt has emerged as an alternative technique to trabeculectomy, which is considered the standard treatment for glaucoma surgery. Currently, it is mainly indicated after failure of trabeculectomy or in some types of glaucoma with high risk of failure. However, there is still controversy regarding its effectiveness compared to trabeculectomy.
METHODS
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS
We identified five systematic reviews including nine studies overall, of which four were randomized trials. We concluded that aqueous shunt might increase the qualified success compared to trabeculectomy, but it is not clear whether it has any effect on the rest of the critical outcomes for decision-making because the certainty of the evidence is very low.
Autores:
Gonzalo Ordenes-Cavieres[1,2], Eduardo Pimentel[1,2], Jimena Schmidt[2,3]
Citación: Ordenes-Cavieres G, Pimentel E, Schmidt J. Aqueous shunt versus trabeculectomy for treatment of glaucoma. Medwave 2018;18(8):e7389 doi: 10.5867/medwave.2018.08.7389
Fecha de envío: 29/11/2018
Fecha de aceptación: 29/12/2018
Fecha de publicación: 19/12/2018
Origen: Este artículo es producto del Epistemonikos Evidence Synthesis Project de la Fundación Epistemonikos, en colaboración con Medwave para su publicación.
Tipo de revisión: Con revisión por pares sin ciego por parte del equipo metodológico del Epistemonikos Evidence Synthesis Project.
Nos complace que usted tenga interés en comentar uno de nuestros artículos. Su comentario será publicado inmediatamente. No obstante, Medwave se reserva el derecho a eliminarlo posteriormente si la dirección editorial considera que su comentario es: ofensivo en algún sentido, irrelevante, trivial, contiene errores de lenguaje, contiene arengas políticas, obedece a fines comerciales, contiene datos de alguna persona en particular, o sugiere cambios en el manejo de pacientes que no hayan sido publicados previamente en alguna revista con revisión por pares.
Aún no hay comentarios en este artículo.
Para comentar debe iniciar sesión
Medwave publica las vistas HTML y descargas PDF por artículo, junto con otras métricas de redes sociales.
Minckler DS, Francis BA, Hodapp EA, Jampel HD, Lin SC, Samples JR, Smith SD, Singh K. Aqueous shunts in glaucoma: a report by the American Academy of Ophthalmology. Ophthalmology. 2008 Jun;115(6):1089-98. | CrossRef | PubMed |HaiBo T, Xin K, ShiHeng L, Lin L. Comparison of Ahmed glaucoma valve implantation and trabeculectomy for glaucoma: a systematic review and meta-analysis. PLoS One. 2015 Feb 26;10(2):e0118142. | CrossRef | PubMed | PMC |Hong CH, Arosemena A, Zurakowski D, Ayyala RS. Glaucoma drainage devices: a systematic literature review and current controversies. Surv Ophthalmol. 2005 Jan-Feb;50(1):48-60. | PubMed |Tice JA. Aqueous shunts for the treatment of glaucoma. California Technology Assessment Forum (CTAF). 2011 Jun. | Link |Tseng VL, Coleman AL, Chang MY, Caprioli J. Aqueous shunts for glaucoma. Cochrane Database Syst Rev. 2017 Jul 28;7:CD004918. | CrossRef | PubMed | PMC |Bluestein EC, Stewart WC. Trabeculectomy with 5-fluorouracil vs single-plate Molteno implantation. Ophthalmic Surg. 1993 Oct;24(10):669-73. | PubMed |Gedde SJ, Schiffman JC, Feuer WJ, Parrish RK 2nd, Heuer DK, Brandt JD; Tube Versus Trabeculectomy Study Group. The tube versus trabeculectomy study: design and baseline characteristics of study patients. Am J Ophthalmol. 2005 Aug;140(2):275-87. | PubMed |Gedde SJ, Herndon LW, Brandt JD, Budenz DL, Feuer WJ, Schiffman JC. Surgical complications in the Tube Versus Trabeculectomy Study during the first year of follow-up. Am J Ophthalmol. 2007 Jan;143(1):23-31. Epub 2006 Sep 1. | PubMed |Gedde SJ, Schiffman JC, Feuer WJ, Herndon LW, Brandt JD, Budenz DL. Treatment outcomes in the tube versus trabeculectomy study after one year of follow-up. Am J Ophthalmol. 2007 Jan;143(1):9-22. | PubMed |Gedde SJ, Schiffman JC, Feuer WJ, Herndon LW, Brandt JD, Budenz DL; Tube Versus Trabeculectomy Study Group. Three-year follow-up of the tube versus trabeculectomy study. Am J Ophthalmol. 2009 Nov;148(5):670-84. doi:https://dx.10.1016/j.ajo.2009.06.018. | PubMed |Gedde SJ, Heuer DK, Parrish RK 2nd; Tube Versus Trabeculectomy Study Group. Review of results from the Tube Versus Trabeculectomy Study. Curr Opin Ophthalmol. 2010 Mar;21(2):123-8. | CrossRef | PubMed | PMC |Gedde SJ, Herndon LW, Brandt JD, Budenz DL, Feuer WJ, Schiffman JC; Tube Versus Trabeculectomy Study Group. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012 May;153(5):804-814.e1. | CrossRef | PubMed | PMC |Gedde SJ, Schiffman JC, Feuer WJ, Herndon LW, Brandt JD, Budenz DL; Tube versus Trabeculectomy Study Group. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. Am J Ophthalmol. 2012 May;153(5):789-803.e2. | CrossRef | PubMed | PMC |Im YWm Lym HS, Park CK, Moon JI. Comparison of Mitomycin C trabeculectomy and Ahmed valve implant surgery for neovascular glaucoma. J Korean Ophthalmol Soc. 2004;45(9):1515-21. | Link |Lee TY, Lee JH, Cha SC. Trabeculectomy with Mitomycin C versus Ahmed valve implantation in pseudophakic glaucomatous eyes. J Korean Ophthalmol Soc. 2008 Feb;49(2):293-302. | Link |Pakravan M, Homayoon N, Shahin Y, Ali Reza BR. Trabeculectomy with mitomycin C versus Ahmed glaucoma implant with mitomycin C for treatment of pediatric aphakic glaucoma. J Glaucoma. 2007 Oct-Nov;16(7):631-6. | PubMed |Rauscher FM, Gedde SJ, Schiffman JC, Feuer WJ, Barton K, Lee RK; Tube Versus Trabeculectomy Study Group. Motility disturbances in the tube versus trabeculectomy study during the first year of follow-up. Am J Ophthalmol. 2009 Mar;147(3):458-66. | CrossRef | PubMed | PMC |Shen CC, Salim S, Du H, Netland PA. Trabeculectomy versus Ahmed Glaucoma Valve implantation in neovascular glaucoma. Clin Ophthalmol. 2011;5:281-6. doi:https://dx.10.2147/OPTH.S16976. | PubMed | PMC |Tran DH, Souza C, Ang MJ, Loman J, Law SK, Coleman AL, Caprioli J. Comparison of long-term surgical success of Ahmed Valve implant versus trabeculectomy in open-angle glaucoma. Br J Ophthalmol. 2009 Nov;93(11):1504-9. | CrossRef | PubMed |Wilson MR, Mendis U, Smith SD, Paliwal A. Ahmed glaucoma valve implant vs trabeculectomy in the surgical treatment of glaucoma: a randomized clinical trial. Am J Ophthalmol. 2000 Sep;130(3):267-73. | PubMed |Wilson MR, Mendis U, Paliwal A, Haynatzka V. Long-term follow-up of primary glaucoma surgery with Ahmed glaucoma valve implant versus trabeculectomy. Am J Ophthalmol. 2003 Sep;136(3):464-70. | PubMed |AOA. Care of the patient with open-angle glaucoma. Optometric clinical practice guideline. 2011. | Link |ICO. Guidelines for glaucoma eye care. International council of ophthalmology guidelines. 2016. | Link |Prum BE Jr, Rosenberg LF, Gedde SJ, Mansberger SL, Stein JD, Moroi SE, Herndon LW Jr, Lim MC, Williams RD. Primary Open-Angle Glaucoma Preferred Practice Pattern(®) Guidelines. Ophthalmology. 2016 Jan;123(1):P41-P111. | CrossRef | PubMed |Gedde SJ, Feuer WJ, Shi W, Lim KS, Barton K, Goyal S, Ahmed IIK, Brandt J; Primary Tube Versus Trabeculectomy Study Group. Treatment Outcomes in the Primary Tube Versus Trabeculectomy Study after 1 Year of Follow-up. Ophthalmology. 2018 May;125(5):650-663. | CrossRef | PubMed |Comparing surgical approaches to treat black African and Africa-caribbean patients with uncontrolled primary open-angle glaucoma: a randomized feasibility study. NCT02989207. | Link |






 Estudios originales
Estudios originales