Revista Biomédica Revisada Por Pares

 Para Descargar PDF debe Abrir sesión.
Para Descargar PDF debe Abrir sesión.
Palabras clave: Laparoscopic appendectomy, open appendectomy, appendicitis, Epistemonikos, GRADE.
INTRODUCTION
The treatment of acute appendicitis using laparoscopy reduces the risk of wound infection, hospitalization time and return to normal activity. However, it increases the risk of intra-abdominal abscess, which is one the main complications of complicated appendicitis.
METHODS
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS
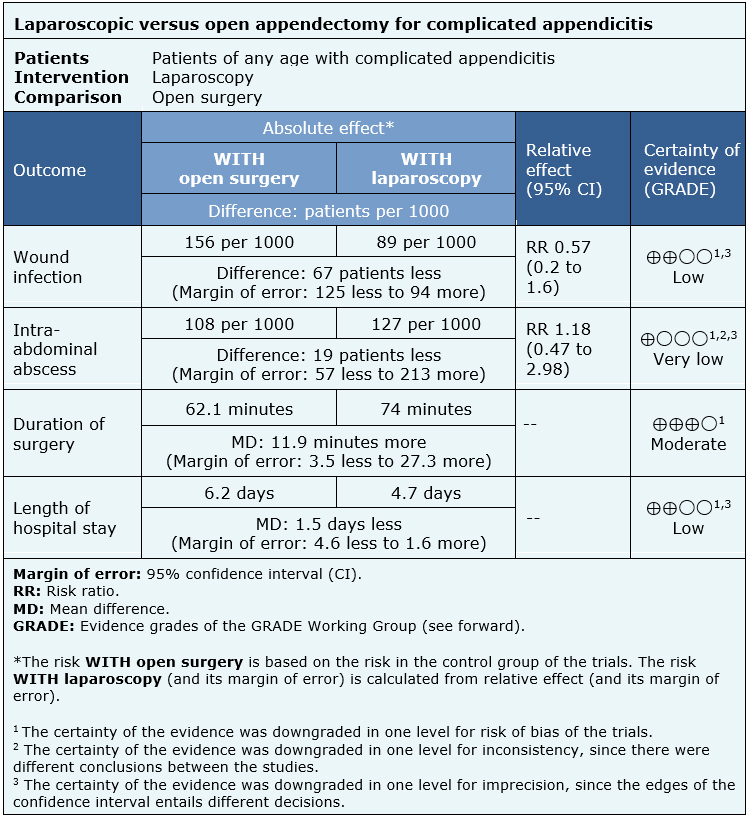
We identified six systematic reviews including 55 studies overall, of which four were randomized trials. We concluded that the used of laparoscopy, compared to open appendectomy, probably reduces the time of hospital stay, and may reduce the risk of wound infection, but there's no clarity regarding the incidence of intra-abdominal abscess due to the very low certainty of the evidence available.
Acute appendicitis remains one of the most common surgical diseases in the emergency room. The lifetime risk might be up to 9% [1],[2]. The treatment of this condition using laparoscopy was first reported in 1983 [3]. The benefits include reduction in the risk of wound infection and the time of hospital stay, and a faster return to normal activity. Because of this, this technique has been well studied and used during the last years. However, one of the disadvantages of this approach is the increased risk of intra-abdominal abscess, particularly in patients presenting with complicated appendicitis. So, there is still controversy about the use of laparoscopy in this setting.
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
|
What is the evidence. |
We identified six systematic reviews [4],[5],[6],[7],[8],[9], including 55 primary studies overall, of which four were randomized trials [10],[11],[12],[13]. This table, and the summary in general, is based on the latter, since the inclusion of the observational studies did not increase the certainty of the evidence or added additional information. |
|
What types of patients were included* |
A total of 857 patients were included in the trials, of which 466 presented complicated appendicitis. Their age ranged from 2 to 85 years. Two trials only included adults [12],[13], one only included children between 2 and 20 years [10] and one implicitly included children, but did not analyze them separately [11]. Male:female ratio was 1.3:1. All trials included patients with complicated appendicitis, which was defined as the presence of intestinal perforation. Only one trial included patients with and without perforation, but presented data separately [10]. |
|
What types of interventions were included* |
Only one trial used 2-handed, 4-trocar technique [12], while the rest used conventional 3-trocar technique. All trials compared against open appendectomy, whether by classic incision (McBurney) or infraumbilical. All trials used an antibiotics scheme pre- and post-surgery. There was no information regarding the level of training of surgeons performing the interventions. |
|
What types of outcomes |
The outcomes measured can be classified into two groups: 1. Technique
2. Post-surgical complications
Patients were monitored for 14-30 days after surgery. |
* The information about primary studies is extracted from the systematic reviews identified, unless otherwise specified.
The information is based on four trials [10],[11],[12],[13], that included 466 patients with complicated appendicitis, of which 197 were treated with laparoscopic appendectomy and 269 with open appendectomy.
All trials reported the length of hospital stay, and three the duration of surgery [11],[12],[13]. All trials measured the incidence of wound infection and intra-abdominal abscess.
The summary of findings is as follows:
| Follow the link to access the interactive version of this table (Interactive Summary of Findings – iSoF) |

|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
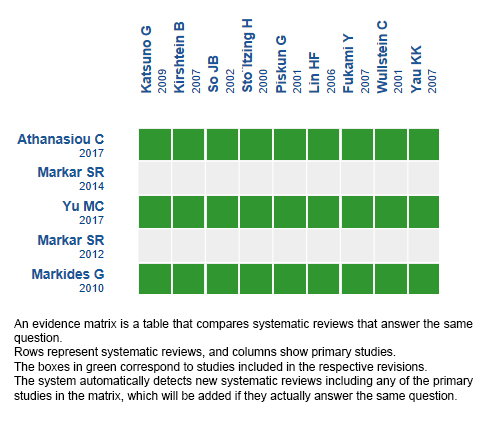
Follow the link to access the interactive version: Laparoscopic versus open appendectomy for complicated appendicitis.
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
 Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
INTRODUCTION
The treatment of acute appendicitis using laparoscopy reduces the risk of wound infection, hospitalization time and return to normal activity. However, it increases the risk of intra-abdominal abscess, which is one the main complications of complicated appendicitis.
METHODS
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS
We identified six systematic reviews including 55 studies overall, of which four were randomized trials. We concluded that the used of laparoscopy, compared to open appendectomy, probably reduces the time of hospital stay, and may reduce the risk of wound infection, but there's no clarity regarding the incidence of intra-abdominal abscess due to the very low certainty of the evidence available.
Autores:
Cristóbal del Pino[1,2], Rodrigo Muńoz[1,3], Gabriel Rada[1,2,4]
Citación: del Pino C, Muńoz R, Rada G. Laparoscopic versus open appendectomy for complicated appendicitis. Medwave 2018;18(8):e7369 doi: 10.5867/medwave.2018.08.7369
Fecha de envío: 10/11/2018
Fecha de aceptación: 27/11/2018
Fecha de publicación: 11/12/2018
Origen: Este artículo es producto del Epistemonikos Evidence Synthesis Project de la Fundación Epistemonikos, en colaboración con Medwave para su publicación.
Tipo de revisión: Con revisión por pares sin ciego por parte del equipo metodológico del Epistemonikos Evidence Synthesis Project.
Nos complace que usted tenga interés en comentar uno de nuestros artículos. Su comentario será publicado inmediatamente. No obstante, Medwave se reserva el derecho a eliminarlo posteriormente si la dirección editorial considera que su comentario es: ofensivo en algún sentido, irrelevante, trivial, contiene errores de lenguaje, contiene arengas políticas, obedece a fines comerciales, contiene datos de alguna persona en particular, o sugiere cambios en el manejo de pacientes que no hayan sido publicados previamente en alguna revista con revisión por pares.
Aún no hay comentarios en este artículo.
Para comentar debe iniciar sesión
Medwave publica las vistas HTML y descargas PDF por artículo, junto con otras métricas de redes sociales.
Crovari Eulufi, F., & Manzor Véliz, M. Manual de patología quirúrgica. Ediciones UC. Anderson JE, Bickler SW, Chang DC et al (2012) Examining a common disease with unknown etiology: trends in epidemiology and surgical management of appendicitis in California, 1995–2009. World J Surg 36:2787–2794. Semm K. Endoscopic appendectomy. Endoscopy. 1983;15:59-64. Athanasiou, C., Lockwood, S., & Markides, G. (2017). Systematic Review and Meta-Analysis of Laparoscopic Versus Open Appendicectomy in Adults with Complicated Appendicitis: an Update of the Literature. World Journal Of Surgery, 41(12), 3083-3099. | CrossRef |Markar, S., Blackburn, S., Karthikesalingam, A., Evans, J., & Kinross, J. (2012). Laparoscopic Versus Open Appendectomy for Complicated and Uncomplicated Appendicitis in Children. Journal Of Gastrointestinal Surgery, 16(10), 1993-2004. | CrossRef |Markar, S., Penna, M., & Harris, A. (2014). Laparoscopic Approach to Appendectomy Reduces the Incidence of Short- and Long-Term Post-operative Bowel Obstruction: Systematic Review and Pooled Analysis. Journal Of Gastrointestinal Surgery, 18(9), 1683-1692. | CrossRef |Markides, G., Subar, D., & Riyad, K. (2010). Laparoscopic Versus Open Appendectomy in Adults with Complicated Appendicitis: Systematic Review and Meta-analysis. World Journal Of Surgery, 34(9), 2026-2040. | CrossRef |Yu, M., Feng, Y., Wang, W., Fan, W., Cheng, H., & Xu, J. (2017). Is laparoscopic appendectomy feasible for complicated appendicitis ?A systematic review and meta-analysis. International Journal Of Surgery, 40, 187-197 | CrossRef |Zhang, S., Du, T., Jiang, X., & Song, C. (2017). Laparoscopic Appendectomy in Children With Perforated Appendicitis. Surgical Laparoscopy, Endoscopy & Percutaneous Techniques, 27(4), 262-266. | CrossRef |Oka, T., Kurkchubasche, A., Bussey, J., Wesselhoeft, C., Tracy, T., & Luks, F. (2004). Open and laparoscopic appendectomy are equally safe and acceptable in children. Surgical Endoscopy, 18(2), 242-245. | CrossRef |Schietroma, M., M.D., Piccione, F., M.D., Carlei, F., M.D., Clementi, M., M.D., Bianchi, Z., M.D., de Vita, F., MD, & Amicucci, G., M.D. (2012). Peritonitis from perforated appendicitis: Stress response after laparoscopic or open treatment. The American Surgeon, 78(5), 582-90. Taguchi, Y., Komatsu, S., Sakamoto, E., Norimizu, S., Shingu, Y., & Hasegawa, H. (2015). Laparoscopic versus open surgery for complicated appendicitis in adults: a randomized controlled trial. Surgical Endoscopy, 30(5), 1705-1712. | CrossRef |Thomson, J., Kruger, D., Jann-Kruger, C., Kiss, A., Omoshoro-Jones, J., Luvhengo, T., & Brand, M. (2014). Laparoscopic versus open surgery for complicated appendicitis: a randomized controlled trial to prove safety. Surgical Endoscopy, 29(7), 2027-2032. | CrossRef |






 Estudios originales
Estudios originales