Revista Biomédica Revisada Por Pares

 Para Descargar PDF debe Abrir sesión.
Para Descargar PDF debe Abrir sesión.
Palabras clave: Non-contrast computed tomography, subarachnoid hemorrhage, Epistemonikos, GRADE.
INTRODUCTION
Subarachnoid hemorrhage is a neurosurgical emergency that requires timely diagnosis due to its severity and the existence of therapeutic measures that are effective when carried out in time. The most used diagnostic sequence to rule it out is computed tomography without contrast which, if negative, is followed by lumbar puncture. However, it has been suggested that a negative non-contrast computed tomography (without blood) may rule out the diagnosis.
METHODS
To answer this question we used Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS
We identified three systematic reviews including nine studies. We concluded the diagnostic accuracy of non-contrast computed tomography is probably very high, but the clinical impact of relying only on this test has not yet been evaluated.
It is estimated that subarachnoid hemorrhage could be responsible for 1% of headaches in emergency services [1],[2]. Its early diagnosis is very important since it is a neurosurgical emergency with very high morbidity and mortality, and there are therapies that can make an important difference if timely implemented [2]. Although it has a characteristic clinical presentation, the symptoms and signs are not enough to rule it out [1],[2]. The most commonly used sequence is non-contrast computed tomography followed by a lumbar puncture, ruling out the condition with both results negative. However, lumbar puncture is not risk-free (infection, hematoma, and stress for the patient) and its added value is a matter of debate [1],[2].
To answer the question, we used Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a section of other considerations for decision-making.
|
Key messages
|
|
What is the evidence. |
We found three systematic reviews [1],[2],[3] that included nine primary studies overall [4],[5],[6],[7],[8],[9],[10],[11],[12], none of them a randomized trial. We did not find studies evaluating the clinical impact. We excluded one systematic review [3] because it mixed non-traumatic with peri-mesencephalic subarachnoid hemorrhage, which is considered a different clinical entity. |
|
What types of patients were included* |
All studies included patients older than 11 years, four studies included adults without specifying age [5],[6],[9],[12] and four studies only included patients without neurological deficit [5],[7],[11],[12]. Five studies evaluated patients with less than 6 hours symptom onset [6],[7],[9],[11],[12], one study with less than 12 hours [5] and three studies did not specify it [4],[8],[10]. One study[6] only included patients with negative non-contrast computed tomography for subarachnoid hemorrhage. |
|
What types of interventions were included* |
Five studies used 16-slice or higher computed tomography [6],[7],[9],[11],[12] and the others did not described the type of computed tomography used[4],[5],[8],[10]. As gold standard, six studies used lumbar puncture, imaging, and follow-up[6],[7],[8],[9],[11],[12] and the rest did not reported it [4],[5],[10]. Five studies followed all of their patients [6],[7][8],[9],[11], three studies did not follow up patients [4],[5],[10] and one study had an incomplete follow up (86% of patients)[12]. |
|
What types of outcomes |
The different systematic reviews pooled outcomes as follows: specificity, sensitivity, positive likelihood ratio (LR +), negative likelihood ratio (LR -), true positives, false negatives, false positives and true negatives. |
* The information about primary studies is extracted from the systematic reviews identified, unless otherwise specified.
Information on the diagnostic accuracy of non-contrast computed tomography for non-traumatic subarachnoid hemorrhage is based on 9 primary studies [5],[6],[7],[8],[9],[10],[11],[12],[13]. All of these measured specificity, sensitivity, LR + and LR- of the non-contrast computed tomography for non-traumatic subarachnoid hemorrhage.
The summary of the findings is as follows:
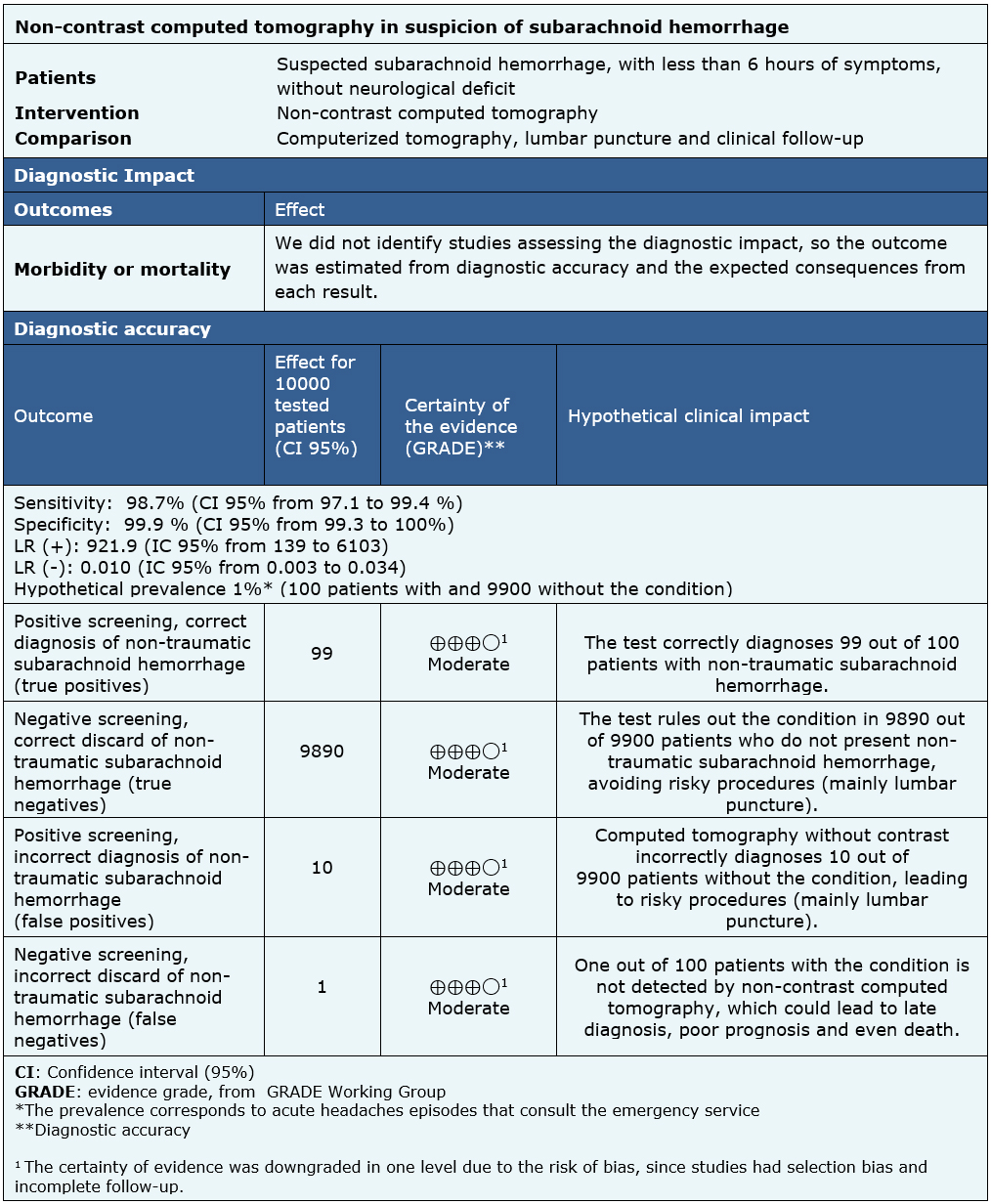
| Follow the link to access the interactive version of this table (Interactive Summary of Findings – iSoF) |

|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
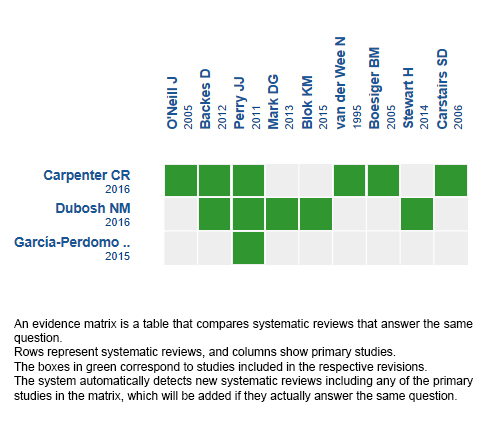
Follow the link to access the interactive version: Accuracy of computed tomography without contrast for the diagnosis of non-traumatic subarachnoid hemorrhage
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
 Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
INTRODUCTION
Subarachnoid hemorrhage is a neurosurgical emergency that requires timely diagnosis due to its severity and the existence of therapeutic measures that are effective when carried out in time. The most used diagnostic sequence to rule it out is computed tomography without contrast which, if negative, is followed by lumbar puncture. However, it has been suggested that a negative non-contrast computed tomography (without blood) may rule out the diagnosis.
METHODS
To answer this question we used Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS
We identified three systematic reviews including nine studies. We concluded the diagnostic accuracy of non-contrast computed tomography is probably very high, but the clinical impact of relying only on this test has not yet been evaluated.
Autores:
Yerko Suazo[1,2], Gabriel Rada[2,3,4,5,6]
Citación: Suazo Y, Rada G. Non-contrast computed tomography for the diagnosis of non-traumatic subarachnoid hemorrhage. Medwave 2018;18(7):e7321 doi: 10.5867/medwave.2018.07.7321
Fecha de envío: 3/6/2018
Fecha de aceptación: 10/9/2018
Fecha de publicación: 7/11/2018
Origen: Este artículo es producto del Epistemonikos Evidence Synthesis Project de la Fundación Epistemonikos, en colaboración con Medwave para su publicación.
Tipo de revisión: Con revisión por pares sin ciego por parte del equipo metodológico del Epistemonikos Evidence Synthesis Project.
Nos complace que usted tenga interés en comentar uno de nuestros artículos. Su comentario será publicado inmediatamente. No obstante, Medwave se reserva el derecho a eliminarlo posteriormente si la dirección editorial considera que su comentario es: ofensivo en algún sentido, irrelevante, trivial, contiene errores de lenguaje, contiene arengas políticas, obedece a fines comerciales, contiene datos de alguna persona en particular, o sugiere cambios en el manejo de pacientes que no hayan sido publicados previamente en alguna revista con revisión por pares.
Aún no hay comentarios en este artículo.
Para comentar debe iniciar sesión
Medwave publica las vistas HTML y descargas PDF por artículo, junto con otras métricas de redes sociales.
Dubosh NM, Bellolio MF, Rabinstein AA, Edlow JA. Sensitivity of Early Brain Computed Tomography to Exclude Aneurysmal Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis. Stroke; a journal of cerebral circulation. 2016;47(3):750-5. Carpenter CR, Hussain AM, Ward MJ, Zipfel GJ, Fowler S, Pines JM, Sivilotti ML. Spontaneous Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis Describing the Diagnostic Accuracy of History, Physical Exam, Imaging, and Lumbar Puncture with an Exploration of Test Thresholds. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2016;23(9):963-1003. García-Perdomo HA, Peńa E, Abello AL. Conventional brain computed tomography for the diagnosis of nontraumatic subarachnoid hemorrhage: A systematic review. Revista Gastrohnup. 2015;17(1):25-32. O'Neill J, McLaggan S, Gibson R. Acute headache and subarachnoid haemorrhage: a retrospective review of CT and lumbar puncture findings. Scottish medical journal. 2005;50(4):151-3. van der Wee N, Rinkel GJ, Hasan D, van Gijn J. Detection of subarachnoid haemorrhage on early CT: is lumbar puncture still needed after a negative scan?. Journal of neurology, neurosurgery, and psychiatry. 1995;58(3):357-9. Mark DG, Hung YY, Offerman SR, Rauchwerger AS, Reed ME, Chettipally U, Vinson DR, Ballard DW, Kaiser Permanente CREST Network Investigators. Nontraumatic subarachnoid hemorrhage in the setting of negative cranial computed tomography results: external validation of a clinical and imaging prediction rule. Annals of emergency medicine. 2013;62(1):1-10.e1. Backes D, Rinkel GJ, Kemperman H, Linn FH, Vergouwen MD. Time-dependent test characteristics of head computed tomography in patients suspected of nontraumatic subarachnoid hemorrhage. Stroke. 2012;43(8):2115-9. Boesiger BM, Shiber JR. Subarachnoid hemorrhage diagnosis by computed tomography and lumbar puncture: are fifth generation CT scanners better at identifying subarachnoid hemorrhage?. The Journal of emergency medicine. 2005;29(1):23-7. Stewart H, Reuben A, McDonald J. LP or not LP, that is the question: gold standard or unnecessary procedure in subarachnoid haemorrhage?. Emergency medicine journal : EMJ. 2014;31(9):720-3. Carstairs SD, Tanen DA, Duncan TD, Nordling OB, Wanebo JE, Paluska TR, Theodore N, Riffenburgh RH. Computed tomographic angiography for the evaluation of aneurysmal subarachnoid hemorrhage. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2006;13(5):486-92. Blok KM, Rinkel GJ, Majoie CB, Hendrikse J, Braaksma M, Tijssen CC, Wong YY, Hofmeijer J, Extercatte J, Kerklaan B, Schreuder TH, ten Holter S, Verheul F, Harlaar L, Pruissen DM, Kwa VI, Brouwers PJ, Remmers MJ, Schonewille WJ, Kruyt ND, Vergouwen MD. CT within 6 hours of headache onset to rule out subarachnoid hemorrhage in nonacademic hospitals. Neurology. 2015;84(19):1927-32. Perry JJ, Stiell IG, Sivilotti ML, Bullard MJ, Emond M, Symington C, Sutherland J, Worster A, Hohl C, Lee JS, Eisenhauer MA, Mortensen M, Mackey D, Pauls M, Lesiuk H, Wells GA. Sensitivity of computed tomography performed within six hours of onset of headache for diagnosis of subarachnoid haemorrhage: prospective cohort study. BMJ (Clinical research ed.). 2011;343:d4277. Ward, M. J., Bonomo, J. B., Adeoye, O., Raja, A. S. and Pines, J. M. (2012), Cost-effectiveness of Diagnostic Strategies for Evaluation of Suspected Subarachnoid Hemorrhage in the Emergency Department. Academic Emergency Medicine, 19: 1134–1144. Connolly ES Jr, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, Hoh BL, Kirkness CJ, Naidech AM, Ogilvy CS, Patel AB, Thompson BG, Vespa P ; on behalf of the American Heart Association Stroke Council; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; Council on Cardiovascular Surgery and Anesthesia; Council on Clinical Cardiology. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association.Stroke. 2012;43:1711–1737. | CrossRef |Steiner T, Juvela S, Unterberg A, Jung C, Forsting M, Rinkel G, European Stroke Organization Guidelines for the Management of Intracranial Aneurysms and Subarachnoid Haemorrhage. Cerebrovasc Dis 2013;35:93-112. Sidman R, Connolly E, Lemke T. Subarachnoid hemorrhage diagnosis: lumbar puncture is still needed when the computed tomography scan is normal. Acad Emerg Med. 1996; 3:827–31. Midhun Mohan, Ola Rominiyi, Aswin Chari Chari. Subarachnoid haemorrhage with negative initial neurovascular imaging: a systematic review and meta-analysis of delayed diagnoses and clinical outcomes. PROSPERO 2016 CRD42016035376. | CrossRef | Link |Dailler F et al. Observational Study of Patients With Subarachnoid Hemorrhage (ProReSHA). WHO, Clinical Trials Registry Platform. NCT02890004. | Link |






 Estudios originales
Estudios originales