Revista Biomķdica Revisada Por Pares

 Para Descargar PDF debe Abrir sesi¾n.
Para Descargar PDF debe Abrir sesi¾n.
Palabras clave: asthma, chronic obstructive pulmonary disease, metered dose inhaler, age factors
BACKGROUND
Inhalation therapy has proven to be the best way to control the asthma and chronic obstructive pulmonary disease symptoms. The most commonly used delivery system to control these symptoms is the metered-dose inhaler. The primary goal of this study is to demonstrate an association between incorrect inhaler use and patient age.
METHODS
This is a cross-sectional study, performed at Centro Mķdico Naval ōCirujano Mayor Santiago Tßvaraö, in Callao, Peru, in 2014. Patients older than 18 years that used metered-dose inhalers were included. We used film recordings of patients using a metered-dose inhaler and compared their technique with the recommendations on the guidelines on the correct use of inhalers of the Spanish Society of Pneumology and Thoracic Surgery (SEPAR). The main variables measured were age and incorrect inhaler use. The results were analyzed with the Chi squared test for bivariate analysis, and for multivariate analysis we used the Poisson regression model with robust variance.
RESULTS
We included 378 patients in the analysis; 167 were older than 60 years. An association was found between incorrect inhalator technique and age (p=0.014) (PR 1.19 95% CI 1.03 to 1.37). The highest prevalence of incorrect technique was found in the young adult population (88%). There was no association between the incorrect technique and the person who taught it (p=0.114). Finally, this study showed that 81.2% of the study population presented an incorrect inhalation technique.
CONCLUSIONS
The percentage of incorrect inhaler use, in the general population is high. Even if we found no association between an incorrect technique and the person who taught it; still, there is a high percentage of errors and it was even demonstrated that being instructed by a pulmonologist does not guarantee a correct performance of metered-dose inhaler inhalations.
Asthma and chronic obstructive pulmonary disease affect the lower respiratory tract. Both have similarities, such as, aerial flow limitation and reactive airways disease [1],[2]. The Global Initiative for Asthma informs that asthma affects between 1 and 18% of world population [1]. The Global Initiative for Chronic Obstructive Pulmonary Disease, classifies chronic obstructive pulmonary disease as the fourth leading cause of death worldwide [2]. According to the World Health Organization (WHO), three million people died because of this disease in 2005 [3].
Amongst medical treatments, inhalation therapy has proven to be the fastest and most efficient toalleviate the symptoms. For this reason, the Global Initiative for Asthma and Global Initiative for Chronic Obstructive Lung Disease recommend the chosen treatment -in most cases- to be by inhalation [1],[2].
There are several inhaling devices. The most common being the pressurized cartridge, whose technical denomination is metered-dose inhaler (MDI) [4],[5],[6],[7].
According to the SEPAR (Spanish Pulmonology and Thoracic Surgery Society), inhalation therapy with the metered-dose inhaler requires a series of steps, three of them important to consider the technique as correct [4],[5],[7],[8].
Previous studies note that error frequencies in the inhalation therapy are demonstrated in around 40% of asthma patients and chronic obstructive pulmonary disease [5]. It is known that a bad technique leads to a bad disease control [2],[9]. In correlation to this, the error rate increases with age [5],[10]. Researches have reported that elderly patients (≥60 years) make the most mistakes in the execution of the inhalation therapy steps [11],[12]. The most common among these mistakes is the lack of coordination between pressing and breathing in the medicine [13],[14].
On the other hand, there has been research to identify who are the leading inhalation technique instructors. It turns out that the technique is taught by nurses, specialists, technicians and residents [15],[16],[17],[18].
There was a study in Peru in 1992, in which the inhalation technique was assessed in three different age groups (group A, under 13 years old; group B, 13 to 60 years old; and group C, over 60 years old). In the results, it was stablished that the geriatric population has a tendency to use the inhaler incorrectly (61%). Nonetheless, the said study did not look for the association between patient age and inhaler technique performance [19].
For this reason, the primary goal of this study is to demonstrate the association between the incorrect inhaler use and patient age of the Department of Pulmonology at Centro Médico Naval, “Cirujano Mayor Santiago Távara”, in Callao, Peru.
This is a cross-sectional, observational and analytical study. It was performed at the Department of Pulmonology of the Centro Médico Naval, “Cirujano Mayor Santiago Távara”, which has a program for asthma and/or chronic obstructive pulmonary disease patients. The study population was composed of patients in this program, attending consultation between April and December, 2014.
The sample design was not probabilistic by convenience. The EPITABLE program was used to calculate the necessary sample size, assuming an 80% power and a 0.05 significance level. A 16% difference between adults and seniors found by Rootmensen et al. [5] was used as reference. A 10% rejection rate and a 10% of incomplete interviews were added, thus obtaining a necessary minimum sample of 378 patients.
Patients with asthma and/or chronic obstructive pulmonary disease, with a minimum age of 18 years and using a metered-dose inhaler were included. Patients using any supplementary device aside from metered-dose inhalers (spacers), the hearing impaired, with cognitive damage defined by medical record, with functional dependency and/or movement disorders were excluded from this study. Also, interviews and badly-filled verification lists were eliminated.
It was stablished the dependent variable to be bad inhalation technique, defined as the patient’s inability to complete at least one of the important steps suggested by the SEPAR (previous preparation to inhaling, pressing the device, and after inhalation). The independent variable was patient age, divided in three categories: young adult (18-39 years), adult (40-59 years), and senior (≥60 years) [20]. Sociodemographic variables were also added, such as sex, education level, marital status and the person teaching the technique.
The instruments used to evaluate the inhalation technique, both in theory and practice, were a verification step list and a survey of seven questions. Both were validated by the SEPAR [4]. They were tested in a pilot study of 44 people of similar characteristics in a different hospital in Lima. In both instruments, the steps to evaluate were described and mentioned were the three important steps to consider a correct inhalation technique: breathing out before inhaling, pressing the device only once mid-inhaling and holding the breath after inhaling. It was considered a bad technique if at least one of these steps weren’t achieved. The sociodemographic variables were obtained by means of a survey conducted by the authors.
Data was collected in pulmonology offices, under a pulmonologist supervision. Additionally, it was guaranteed that every patient in consultation met the criteria aforementioned, before chosen to participate in this study. Only one patient refused.
Collection process was divided in four stages. First one was to hand out a consent form, detailing the process and the objective of the study, in order to get the authorization. In the second stage, sociodemographic data was collected and patients were filmed with a digital camera while they performed the inhalation technique. In the third stage, the patient’s know-how abilities were assessed with a survey by the SEPAR. Subsequently, each video was assessed by three pulmonologists, under supervision of the authors. This process was performed in different dates, depending on the availability of the doctors and researchers. The evaluation was performed on the basis of a step verification list validated by the SEPAR. Finally, the evaluations by three specialists were compared and the final result was determined by majority.
For this research, the surveys and videos were coded in order to protect the identity of the patients. The videos are kept in an external device in the custody of one of the authors. This study was approved by the Ethics Committee of the Universidad Peruana de Ciencias Aplicadas and the Centro Médico Naval “Cirujano Mayor Santiago Távara”.
A database was generated in Microsoft Excel by double digitation, afterwards exported to STAVA v11.0 for the statistical analysis. Absolute and relative frequencies of the categorical variables were described. The association between inhalation technique and the assessed variables were measured using Chi-square. Also, crude prevalence reasons were calculated and adjusted using simple Poisson regression models with robust variance. P<0.05 was considered significant.
There were 379 patients included in this study, of which 378 were included in the analysis. The characteristics of this population are shown in Table 1. Within the age group, participants over 60 years old amounted to 44.2% (167). 50.5% (191) of participants were women. In t bivariate analysis, the link between patient age and incorrect inhalation technique was demonstrated (p=0.015). Also, it was found that the young adults group was the one with the most frequent errors when using the inhaler (88%). There was no link between gender, education and person teaching the inhalation technique.
On the other hand, 83.6% of patients previously instructed by a pulmonologist made a mistake in the inhalation technique. Patients instructed by non-medical staff (technicians, nurses, etc.) also obtained a high rate of error frequency similar to patients instructed by a pulmonologist (83.4%).
Table 2 shows the most common mistakes in regards to theoretical knowledge. Amongst them were preparation previous to inhalation and what to do if there is need of a second dose.
Table 2. Theoretical knowledge of inhalation technique and most common mistakes (n=378).
Table 3 shows the most common errors in practicing the inhalation technique, the most common being exhaling before slow inhalation. These steps are considered important for a correct inhalation technique.
Table 3. Execution of inhalation technique and most common mistakes (n=378).
Finally, table 4 shows the multivariate analysis between patient age and incorrect inhalation technique. Poisson regression with robust variance was used due to the high prevalence of incorrect inhalation technique (81.2%). It was demonstrated that a young adult, in comparison to an adult, is most likely to make mistakes in the inhalation technique, both in the crude model and the model adjusted by the following variables: sex, education, marital status and person teaching the technique (PR 1.19 with confidence interval of 95%, 1.03-1.37).
There is an association between patient age and incorrect inhalation technique. Also, being a young adult increases the probability of making mistakes in the technique. This age group showed the most prevalence in this aspect. It was also demonstrated that over half of the study population did not develop a correct inhalation technique. The most common mistakes were exhaling before and slow inhalation, steps considered important to perform a correct inhalation technique. Besides, no significant association between the person teaching the technique and the patient performing it was found.
Researches such as the Rootmensen et al. and the Şen et al., are looking to find the link between technique performance and patient age. This last variable is divided in two categories; adult and senior. These studies do not find a significant association between these variables. Nonetheless, this study proved there is a compelling association between patient age and incorrect technique in relation to young adults (<40 years). This can be attributed to the existence of more programs oriented towards integral welfare for seniors, promoting disease awareness and adhesion to the treatment. Also, these programs recommend get annual check-ups to get reassessed and reoriented regarding correct treatment management [19]. On the other hand, young adult population lacks disease awareness and keeps a fast-paced lifestyle, which prevents them from following the steps for a correct inhalation technique [21].
Then again, it was expected that patients instructed by a pulmonologist had a better performance in comparison to the rest of the population. However, there were no significant differences regarding who teaches the technique, but there was a tendency to a bad performance from people taught by a pulmonologist. This likely occurs because there is no continuous evaluation, as suggested by the Global Initiative for Asthma [1]. This results in a poor performance of the inhalation technique and control of the disease.
A similar frequency of incorrect inhalation technique was found in patients instructed by non-medical staff. This can be attributed to the fact that the staff has basic knowledge of the inhalation technique, not necessarily correct, because teaching it is not part of their work description and thus they are not qualified for it. The lowest frequency of incorrect inhalation technique was demonstrated in the group of patients instructed by geriatric specialists and residents; however, it is still considered high (73.6%). Previous studies have researched the usage of inhaler in residents of general medicine. In those studies, the inhalation technique was assessed and it was found that most do not have a correct technique [15],[16].
Two decades have passed since Rey de Castro and Portocarrero researched in Peru the prevalence of incorrect inhalation technique. The methodology implemented in that study is not clear nor is it specified if the used instrument was validated or what was considered as an incorrect inhalation technique.
It is limited to find the prevalence of incorrect inhaler use. In the results, it was determined that over half of the population was using an incorrect technique (61%). Additionally, this study has determined the persistency of a high frequency of the incorrect use of metered-dose inhaler (81.2%), it has even surpassed the value found in the aforementioned study. It is possible that the lack of consensus regarding the steps to follow is the cause of an incorrect inhalation technique.
In regards to the most common mistakes in relation to the theory and practice, the ones with the highest percentage were the ones considered by the SEPAR as important to perform a correct inhalation technique [4]. These results coincide with other studies [5],[7][8],[18], which is an important piece of information since these steps allow for a better medicine distribution.
As for the limitations, it is considered that the study was conducted at an army hospital, given that it counts with a controlled population and its characteristics might be different to the general public. This is due to the fact that they have a more homogenous instruction level and higher economic incomes. Also, the design of the sample was not probabilistic, the results of this study are not comparable. On the other hand, there is no information about the disease time, which would have proven if said variable affects the correct usage of metered-dose inhalers.
The frequency of incorrect inhalation technique is high in the general population. In the young adult group there exists a higher probability of incorrectly performing the technique. The ones responsible for teaching the patient do not teach it in a suitable manner, it was even demonstrated that the patients instructed by a pulmonologist were the ones with the worst performance. Finally, the most common mistakes found in this population coincide with the ones found in other articles.
With this in mind, it is necessary to conduct studies that assess the knowledge and performance in regards to inhalation technique and the professionals in charge of teaching it. This with the objective of taking preventative measures focused on the continuous training said professionals. It is also suggested to research more extensively the link between the inhalation technique and the age group that had most mistakes performing it.
Lastly, it is recommended to evaluate the patients continuously, especially the young adult group, in order to identify errors in metered-dose inhaler use and address them in a correct manner in order to accomplish a correct management of the disease.
Declaration of conflicts of interest
The authors have completed the conflicts of interest form of the International Committee of Medical Journal Editors (ICMJE), translated to Spanish by Medwave and declare not to have received funding for the realization of the study and not to have conflicts of interest associated to its content. The forms may be requested to the author or the editorial address of the Journal.
Ethical aspects
The Journal has evidence that the study was approved by the Ethics Committee of the Health Sciences School of the Universidad de Ciencias Aplicadas
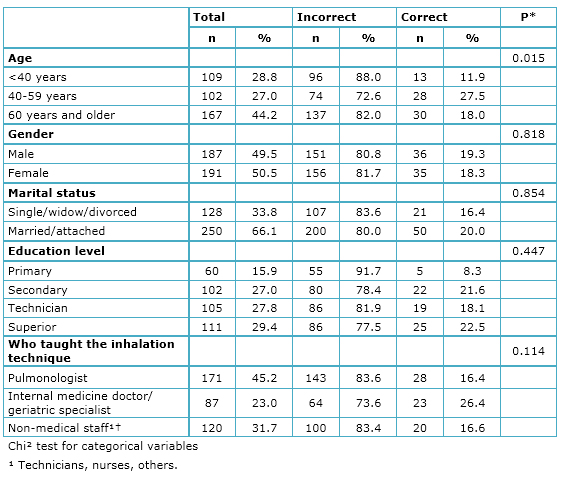 Table 1. Population characteristics and factors associated to the incorrect inhalation technique (n=378).
Table 1. Population characteristics and factors associated to the incorrect inhalation technique (n=378).
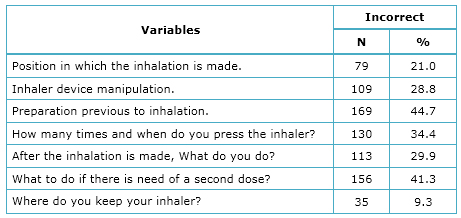 Table 2. Theoretical knowledge of inhalation technique and most common mistakes (n=378).
Table 2. Theoretical knowledge of inhalation technique and most common mistakes (n=378).
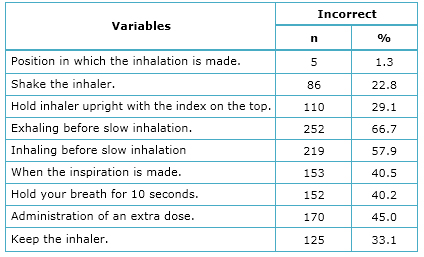 Table 3. Execution of inhalation technique and most common mistakes (n=378).
Table 3. Execution of inhalation technique and most common mistakes (n=378).
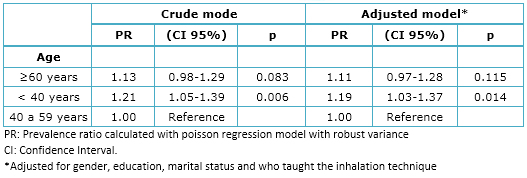 Table 4. Results of the Poisson regression model with robust variance to evaluate the association between patient age and incorrect inhalation technique.
Table 4. Results of the Poisson regression model with robust variance to evaluate the association between patient age and incorrect inhalation technique.
 Esta obra de Medwave estß bajo una licencia Creative Commons Atribuci¾n-NoComercial 3.0 Unported. Esta licencia permite el uso, distribuci¾n y reproducci¾n del artĒculo en cualquier medio, siempre y cuando se otorgue el crķdito correspondiente al autor del artĒculo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave estß bajo una licencia Creative Commons Atribuci¾n-NoComercial 3.0 Unported. Esta licencia permite el uso, distribuci¾n y reproducci¾n del artĒculo en cualquier medio, siempre y cuando se otorgue el crķdito correspondiente al autor del artĒculo y al medio en que se publica, en este caso, Medwave.
BACKGROUND
Inhalation therapy has proven to be the best way to control the asthma and chronic obstructive pulmonary disease symptoms. The most commonly used delivery system to control these symptoms is the metered-dose inhaler. The primary goal of this study is to demonstrate an association between incorrect inhaler use and patient age.
METHODS
This is a cross-sectional study, performed at Centro Mķdico Naval ōCirujano Mayor Santiago Tßvaraö, in Callao, Peru, in 2014. Patients older than 18 years that used metered-dose inhalers were included. We used film recordings of patients using a metered-dose inhaler and compared their technique with the recommendations on the guidelines on the correct use of inhalers of the Spanish Society of Pneumology and Thoracic Surgery (SEPAR). The main variables measured were age and incorrect inhaler use. The results were analyzed with the Chi squared test for bivariate analysis, and for multivariate analysis we used the Poisson regression model with robust variance.
RESULTS
We included 378 patients in the analysis; 167 were older than 60 years. An association was found between incorrect inhalator technique and age (p=0.014) (PR 1.19 95% CI 1.03 to 1.37). The highest prevalence of incorrect technique was found in the young adult population (88%). There was no association between the incorrect technique and the person who taught it (p=0.114). Finally, this study showed that 81.2% of the study population presented an incorrect inhalation technique.
CONCLUSIONS
The percentage of incorrect inhaler use, in the general population is high. Even if we found no association between an incorrect technique and the person who taught it; still, there is a high percentage of errors and it was even demonstrated that being instructed by a pulmonologist does not guarantee a correct performance of metered-dose inhaler inhalations.
Autores:
Alexandra Cayo-Qui±e[1], Valeria MartĒnez-Vargas[1], Rossi Bustamante-Voysest[1], Alejandro Piscoya[1], Yeny Alberca[2]
Citaci¾n: Cayo-Qui±e A, MartĒnez-Vargas V, Bustamante-Voysest R, Piscoya A, Alberca Y. Incorrect use of metered-dose inhalers in adult patients at a hospital in Callao, Peru, 2014: cross-sectional study. Medwave 2015;15(5):e6163 doi: 10.5867/medwave.2015.05.6163
Fecha de envĒo: 15/4/2015
Fecha de aceptaci¾n: 5/6/2015
Fecha de publicaci¾n: 17/6/2015
Origen: no solicitado
Tipo de revisi¾n: con revisi¾n por cuatro pares revisores externos, a doble ciego
Nos complace que usted tenga interķs en comentar uno de nuestros artĒculos. Su comentario serß publicado inmediatamente. No obstante, Medwave se reserva el derecho a eliminarlo posteriormente si la direcci¾n editorial considera que su comentario es: ofensivo en alg·n sentido, irrelevante, trivial, contiene errores de lenguaje, contiene arengas polĒticas, obedece a fines comerciales, contiene datos de alguna persona en particular, o sugiere cambios en el manejo de pacientes que no hayan sido publicados previamente en alguna revista con revisi¾n por pares.
A·n no hay comentarios en este artĒculo.
Para comentar debe iniciar sesi¾n
Medwave publica las vistas HTML y descargas PDF por artĒculo, junto con otras mķtricas de redes sociales.
Bateman E, Boulet L, Cruz A, Fitzgerald M, Haahtela T, Levy M, et al. Global Strategy for Asthma Management and Prevention. Recommendations GINA. USA; 2014. | Link |Rodriguez-Rosin R, Anzueto A, Bourbeau J, deGuia T, Hui D, Martinez F, et al. Guide to COPD Diagnosis, Management And Prevention. Global Initiative for Chronic Obstructive Lung Disease. Recommendations GOLD. USA; 2011. | Link |Donaire J, Basualdo V, Casan P, Hernßndez C, Macißn V, et al. Normativa 22. Utilizacion de fßrmacos inhalados. Recomendaciones SEPAR. Espa±a; 2011. | Link |Rootmensen GN, van Keimpema AR, Jansen HM, de Haan RJ. Predictors of incorrect inhalation technique in patients with asthma or COPD: a study using a validated videotaped scoring method. J Aerosol Med Pulm Drug Deliv. 2010 Oct;23(5):323-8. | CrossRef | PubMed |Coelho AC, Souza-Machado A, Leite M, Almeida P, Castro L, Cruz CS, et al. Use of inhaler devices and asthma control in severe asthma patients at a referral center in the city of Salvador, Brazil. J Bras Pneumol. 2011 Nov-Dec;37(6):720-8. | PubMed |Alba G, L¾pez Sßnchez S, Ramos J, GarcĒa G, Clopķs Estela A, Bonal de Falgas J. Valoraci¾n de los conocimientos y utilizaci¾n de inhaladores en pacientes hospitalizados. Farm Hosp.1999;23(5):307-312.
| Link |Hesselink AE, Penninx BW, Wijnhoven HA, Kriegsman DM, van Eijk JT. Determinants of an incorrect inhalation technique in patients with asthma or COPD. Scand J Prim Health Care. 2001 Dec;19(4):255-60.
| PubMed |Joels C. Protocol for assessing inhaler technique in patients with asthma.Nurs Stand. 2012 Jan 11-17;26(19):43-7. | PubMed |Khassawneh BY, Al-Ali MK, Alzoubi KH, Batarseh MZ, Al-Safi SA, Sharara AM, et al. Handling of inhaler devices in actual pulmonary practice: metered-dose inhaler versus dry powder inhalers. Respir Care. 2008 Mar;53(3):324-8. | PubMed |Şen E, G÷n³ll³ U, Ekici Z, Kurşun N. Assessment of inhaler technique and treatment compliance of hospitalized patients and outpatients in a university hospital. Ankara ▄niversitesi Tıp Fak³ltesiMecmuası. 2006; 59:1-6. | Link |Ho SF, OMahony MS, Steward JA, Breay P, Burr ML. Inhaler technique in older people in the community. Age Ageing. 2004 Mar;33(2):185-8. | PubMed |Stelmach R, Robles-Ribeiro PG, Ribeiro M, Oliveira JC, Scalabrini A, Cukier A. Incorrect application technique of metered dose inhalers by internal medicine residents: impact of exposure to a practical situation. J Asthma. 2007 Nov;44(9):765-8 | PubMed |Barbosa J, Padovani C, Godoy I. Inhaled medication on asthma management: evaluation of how asthma patients, medical students, and doctors use the different devices. J Pneumologia.2003;29 (2):75-81. | CrossRef |Kim SH, Kwak HJ, Kim TB, Chang YS, Jeong JW, Kim CW, et al. Inappropriate techniques used by internal medicine residents with three kinds of inhalers (a metered dose inhaler, Diskus, and Turbuhaler): changes after a single teaching session. J Asthma. 2009 Nov;46(9):944-50.
| CrossRef | PubMed |Sotomayor H, Vera A, Naveas R, Sotomayor C. [Assessment of techniques and errors in the use of metered dose inhalers in the adult patient]. Rev Med Chil. 2001 Apr;129(4):413-20. | PubMed |Rey de Castro J, Portocarrero B. Uso adecuado de inhaladores dosificados. Evaluaci¾n en 250 pacientes. Bol Soc Peruana Medicina Inter. 1992;5(3). | Link |Ministerio de Salud, Per·, Cuidados y autocuidado de la Salud. Personas Adultas Mayores. Per·: MINSA; 2011. Chavez J, Lozano M, Lara A. Velasquez O. La actividad fĒsica y el deporte en el adulto mayor. Mexico; 2011. | Link |






 Estudios originales
Estudios originales