Revista Biomķdica Revisada Por Pares

 Para Descargar PDF debe Abrir sesi¾n.
Para Descargar PDF debe Abrir sesi¾n.
Palabras clave: ulipristal, uterine fibroids, epistemonikos, GRADE
Introduction
Uterine fibroids are frequently encountered in gynecology and are a therapeutic challenge. New therapies, such as ulipristal acetate, could help with symptomatic relief, improve quality of life, and decrease uterine fibroid size. Notwithstanding, there is controversy about adverse effects, especially for hepatotoxicity.
Methods
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis, and generated a summary of findings table using the GRADE approach.
Results and conclusions
We identified nine systematic reviews and included ten studies overall, of which five were randomized trials. We conclude that ulipristal increases the likelihood of amenorrhea, improves the quality of life, and decreases menstrual bleeding. However, there is also a likely increase in the risk of adverse effects. Furthermore, ulipristal could decrease the size of fibroids.
Uterine fibroids have an incidence of 40% in women older than 35 years [1]. They are symptomatic less than 30% of the time, including dysmenorrhea and abnormal uterine bleeding, among the most frequent [2].
Most of the time, these symptoms respond well to medical treatments such as non-steroidal anti-inflammatory drugs or contraceptives. The remaining percentage will eventually require surgery, ranging from myomectomy to hysterectomy. Uterine fibroids account for 60% of major gynecological surgeries [3] and cost between 1,400 and 2,300 USD. When seeking to preserve the patient’s fertility, a myomectomy can be performed, a surgery that generally has high bleeding rates and requires adequate training by the surgeon. Since this technique was described, various preoperative strategies have been tried to reduce bleeding.
Among the different medical alternatives available, ulipristal acetate has been used to reduce bleeding and eventually facilitates surgery [4]. Despite this benefit, there is controversy about its use because adverse events have been described.
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), a meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach, and a table of other considerations for decision-making.
|
Main messages
|
|
What is the evidence |
We identified nine systematic reviews [1],[4],[5],[6],[7],[8],[9],[10],[11] including 11 studies overall[12],[13],[14],[15],[16],[17],[18],[19],[20],[21],[22] of which five were randomized trials [12],[13],[14],[15],[16],[17]. The table and summary are based on the randomized trials, as the observational studies did neither increase the level of certainty of the evidence nor added any additional relevant information. |
|
What types of patients were included* |
All trials included patients with uterine fibroids, which were defined as the presence of at least one fibroid diagnosed by ultrasound [12],[15],[16], or magnetic resonance [13]. One trial did not define the imaging technique for the diagnosis of uterine fibroids [12]. Of these patients, the age range was 18 to 50 years [12],[15],[16],[17], only one trial considered ages 33 to 50 years [13]. Patients in menopause, using progestins or agents that alter ovarian or liver function, as well as a history of previous gynaecological surgery [12],[13],[15],[16],[17], were excluded. In addition, other trials excluded patients using corticosteroids [12],[13],[17], with a history of gynaecological cancer [12],[13],[15],[17], with coagulation disorders [12],[15],[17], a history of polyp and/or endometrial hyperplasia [12],[17], patients with blood transfusions or haemoglobin less than 6 grams per decilitre [12] and use of anticoagulants [12],[17]. |
|
What types of interventions were included* |
All trials used ulipristal as an intervention and were compared with placebo. Three trials [12],[15],[16] used the drug at doses of 5 and 10 milligrams. Only one trial [13] considered doses of 10 and 20 milligrams. Four trials [13],[15],[16],[17] did not report surgery following ulipristal use. One trial [12] did consider surgery following surgery. |
|
What types of outcomes were measured |
All the clinical trials reported multiple outcomes, which were as follows:
Follow-up ranged from 12 [15],[16] to 13 weeks [12]. Only one trial had a follow-up of 90 and 110 days [13]. |
*Information about primary studies is not extracted directly from primary studies but from identified systematic reviews, unless otherwise stated.
Information on the effects of ulipristal acetate on uterine fibroids is based on four randomized trials [12],[13],[15],[16], which included 873 patients.
Four trials measured amenorrhea outcome (862 patients) [12],[13],[15],[16], two trials measured quality of life outcome (195 patients) [13],[16], and one trial measured adverse effects outcome (237 patients) [12]. Only one trial measured reduction in menstruation at doses of 5 and 10 mg (289 patients) [12]. Only one trial measured fibroid reduction [12].
None of the systematic reviews reported pregnancy rates and hepatotoxicity outcomes.
The summary of results is as follows:
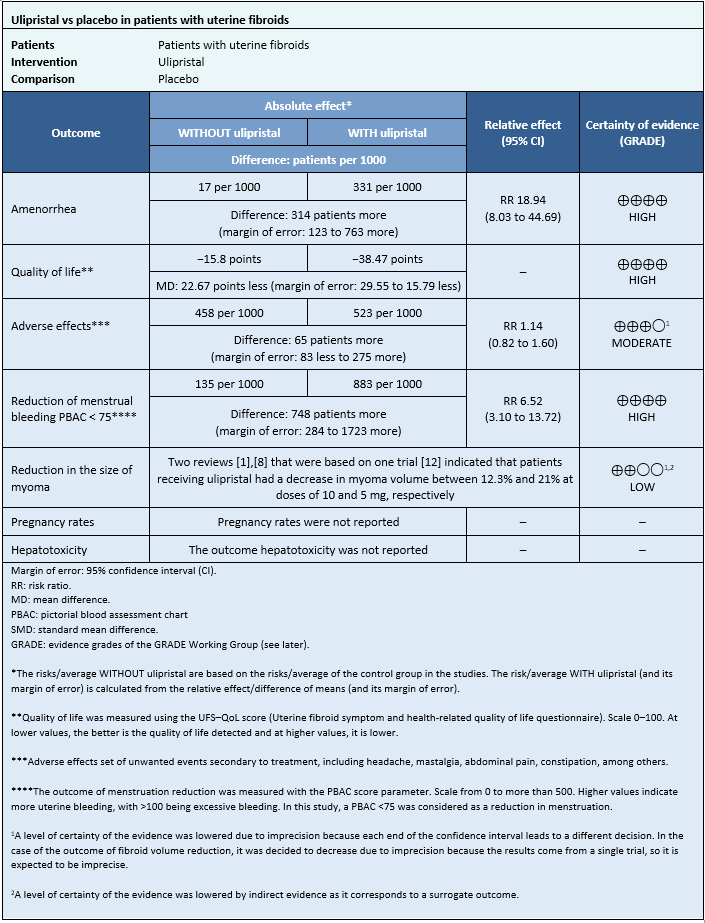
Follow the link to access the interactive version of this table (Interactive Summary of Findings – iSoF)
Other considerations for decision-making
| To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and harms, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
| Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and present it as a matrix of evidence.
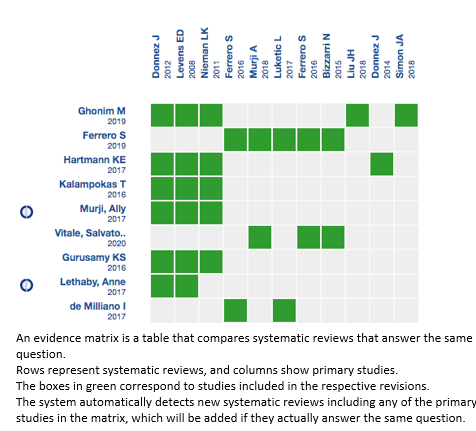
Follow the link to access the interactive version: Ulipristal for uterine fibroids.
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time the new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and an internal peer review process. Each of these articles corresponds to a summary, denominated Friendly Summary of Body of Evidence using Epistemonikos (FRISBEE), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a not-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is the Epistemonikos database.
Roles and contributions
RAD: Conceptualization, investigation, writing (review and editing), and supervision. NNP and MVC: Conceptualization, methodology, analysis, investigation, data curation, writing (review and editing), manuscript preparation (original draft preparation), and visualization.
Competing interests
The authors who completed the ICMJE conflict of interest declared that they did not receive funds for completion of this article; they do not have financial relationships with an organization that may have an interest in the published article and they do not have other relationships or activities that may influence the publication of the article.
Funding
The authors declare Universidad Finis Terrae supported this study.
Ethics
This study was not presented to the ethics committee because the source of information for this review was secondary, and the articles were public.
Language of submission
Spanish.
 Esta obra de Medwave estß bajo una licencia Creative Commons Atribuci¾n-NoComercial 3.0 Unported. Esta licencia permite el uso, distribuci¾n y reproducci¾n del artĒculo en cualquier medio, siempre y cuando se otorgue el crķdito correspondiente al autor del artĒculo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave estß bajo una licencia Creative Commons Atribuci¾n-NoComercial 3.0 Unported. Esta licencia permite el uso, distribuci¾n y reproducci¾n del artĒculo en cualquier medio, siempre y cuando se otorgue el crķdito correspondiente al autor del artĒculo y al medio en que se publica, en este caso, Medwave.
Introduction
Uterine fibroids are frequently encountered in gynecology and are a therapeutic challenge. New therapies, such as ulipristal acetate, could help with symptomatic relief, improve quality of life, and decrease uterine fibroid size. Notwithstanding, there is controversy about adverse effects, especially for hepatotoxicity.
Methods
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis, and generated a summary of findings table using the GRADE approach.
Results and conclusions
We identified nine systematic reviews and included ten studies overall, of which five were randomized trials. We conclude that ulipristal increases the likelihood of amenorrhea, improves the quality of life, and decreases menstrual bleeding. However, there is also a likely increase in the risk of adverse effects. Furthermore, ulipristal could decrease the size of fibroids.
Autores:
Natalia Navarro Plazaola[1], Marla Vega Chacana[1], Raimundo Avilķs Dorlhiac[2]
Citaci¾n: Navarro Plazaola N, Vega Chacana M, Avilķs Dorlhiac R. Effects of ulipristal acetate in patients with symptomatic uterine fibroids. Medwave 2021;21(4):e8162 doi: 10.5867/medwave.2021.04.8162
Fecha de envĒo: 28/10/2020
Fecha de aceptaci¾n: 10/3/2021
Fecha de publicaci¾n: 7/5/2021
Origen: No solicitado
Tipo de revisi¾n: Con revisi¾n por pares externa, por dos ßrbitros a doble ciego
Nos complace que usted tenga interķs en comentar uno de nuestros artĒculos. Su comentario serß publicado inmediatamente. No obstante, Medwave se reserva el derecho a eliminarlo posteriormente si la direcci¾n editorial considera que su comentario es: ofensivo en alg·n sentido, irrelevante, trivial, contiene errores de lenguaje, contiene arengas polĒticas, obedece a fines comerciales, contiene datos de alguna persona en particular, o sugiere cambios en el manejo de pacientes que no hayan sido publicados previamente en alguna revista con revisi¾n por pares.
A·n no hay comentarios en este artĒculo.
Para comentar debe iniciar sesi¾n
Medwave publica las vistas HTML y descargas PDF por artĒculo, junto con otras mķtricas de redes sociales.
Lethaby A, Puscasiu L, Vollenhoven B. Preoperative medical therapy before surgery for uterine fibroids. Cochrane Database Syst Rev. 2017 Nov 15;11(11):CD000547. | CrossRef | PubMed |Buttram VC Jr, Reiter RC. Uterine leiomyomata: etiology, symptomatology, and management. Fertil Steril. 1981 Oct;36(4):433-45. | CrossRef | PubMed |Carls GS, Lee DW, Ozminkowski RJ, Wang S, Gibson TB, Stewart E. What are the total costs of surgical treatment for uterine fibroids? J Womens Health (Larchmt). 2008 Sep;17(7):1119-32. | CrossRef | PubMed |Murji A, Whitaker L, Chow TL, Sobel ML. Selective progesterone receptor modulators (SPRMs) for uterine fibroids. Cochrane Database Syst Rev. 2017 Apr 26;4(4):CD010770. | CrossRef | PubMed |de Milliano I, Twisk M, Ket JC, Huirne JA, Hehenkamp WJ. Pre-treatment with GnRHa or ulipristal acetate prior to laparoscopic and laparotomic myomectomy: A systematic review and meta-analysis. PLoS One. 2017 Oct 16;12(10):e0186158. | CrossRef | PubMed |Ghonim M, Magdy R, Sabbour M, Ghonim M, Nabhan A. A systematic review and meta-analysis of ulipristal acetate for symptomatic uterine fibroids. Int J Gynaecol Obstet. 2019 Aug;146(2):141-148. | CrossRef | PubMed |Ferrero S, Vellone VG, Barra F, Scala C. Ulipristal Acetate before Hysteroscopic and Laparoscopic Surgery for Uterine Myomas: Help or Hindrance?
Gynecol Obstet Invest. 2019;84(4):313-325. | CrossRef | PubMed |Kalampokas T, Kamath M, Boutas I, Kalampokas E. Ulipristal acetate for uterine fibroids: a systematic review and meta-analysis. Gynecol Endocrinol. 2016;32(2):91-6. | CrossRef | PubMed |Vitale SG, Ferrero S, Caruso S, Barra F, MarĒn-Buck A, Vilos GA, et al. Ulipristal Acetate Before Hysteroscopic Myomectomy: A Systematic Review. Obstet Gynecol Surv. 2020 Feb;75(2):127-135. | CrossRef | PubMed |Hartmann KE, Fonnesbeck C, Surawicz T, et al. Management of Uterine Fibroids. Rockville (MD): Agency for Healthcare Research and Quality (US); 2017 | Link |Gurusamy KS, Vaughan J, Fraser IS, Best LM, Richards T. Medical Therapies for Uterine Fibroids - A Systematic Review and Network Meta-Analysis of Randomised Controlled Trials. PLoS One. 2016 Feb 26;11(2):e0149631. | CrossRef | PubMed |Donnez J, Tatarchuk TF, Bouchard P, Puscasiu L, Zakharenko NF, Ivanova T, et al. Ulipristal acetate versus placebo for fibroid treatment before surgery. N Engl J Med. 2012 Feb 2;366(5):409-20. | CrossRef | PubMed |Nieman LK, Blocker W, Nansel T, Mahoney S, Reynolds J, Blithe D, et al. Efficacy and tolerability of CDB-2914 treatment for symptomatic uterine fibroids: a randomized, double-blind, placebo-controlled, phase IIb study. Fertil Steril. 2011 Feb;95(2):767-72.e1-2. | CrossRef | PubMed |Levens ED, Potlog-Nahari C, Armstrong AY, Wesley R, Premkumar A, Blithe DL, et al. CDB-2914 for uterine leiomyomata treatment: a randomized controlled trial. Obstet Gynecol. 2008 May;111(5):1129-36. | CrossRef | PubMed |Liu JH, Soper D, Lukes A, Gee P, Kimble T, Kroll R, et al. Ulipristal Acetate for Treatment of Uterine Leiomyomas: A Randomized Controlled Trial. Obstet Gynecol. 2018 Nov;132(5):1241-1251. | CrossRef | PubMed |Simon JA, Catherino W, Segars JH, et al. Ulipristal Acetate for Treatment of Symptomatic Uterine Leiomyomas: A Randomized Controlled Trial. Obstet Gynecol. 2018;131(3):431-439. | CrossRef |Donnez J, Vßzquez F, Tomaszewski J, Nouri K, Bouchard P, Fauser BC, et al. Long-term treatment of uterine fibroids with ulipristal acetate ☆. Fertil Steril. 2014 Jun;101(6):1565-73.e1-18. | CrossRef | PubMed |Bizzarri N, Ghirardi V, Remorgida V, Venturini PL, Ferrero S. Three-month treatment with triptorelin, letrozole and ulipristal acetate before hysteroscopic resection of uterine myomas: prospective comparative pilot study. Eur J Obstet Gynecol Reprod Biol. 2015 Sep;192:22-6. | CrossRef | PubMed |Ferrero S, Racca A, Tafi E, Alessandri F, Venturini PL, Leone Roberti et al. Ulipristal Acetate Before High Complexity Hysteroscopic Myomectomy:
A Retrospective Comparative Study. J Minim Invasive Gynecol. 2016 Mar-Apr;23(3):390-5. | CrossRef | PubMed |Murji A, Wais M, Lee S, Pham A, Tai M, Liu G. A Multicenter Study Evaluating the Effect of Ulipristal Acetate during Myomectomy. J Minim Invasive Gynecol. 2018 Mar-Apr;25(3):514-521. | CrossRef | PubMed |Luketic L, Shirreff L, Kives S, Liu G, El Sugy R, Leyland N, et al. Does Ulipristal Acetate Affect Surgical Experience at Laparoscopic Myomectomy? J Minim Invasive Gynecol. 2017 Jul-Aug;24(5):797-802. | CrossRef | PubMed |Ferrero S, Alessandri F, Vellone VG, Venturini PL, Leone Roberti Maggiore U. Three-month treatment with ulipristal acetate prior to laparoscopic myomectomy of large uterine myomas: a retrospective study. Eur J Obstet Gynecol Reprod Biol. 2016 Oct;205:43-7. | CrossRef | PubMed |Keown A. FDA Rejects Allergan's Uterine Fibroid Treatment Following EMA Concerns Over Liver Damage. BioSpace. 2018. [On line] | Link |AEMPS 2018. ESMYA (Acetato de ulipristal): Restricciones de uso y nuevas medidas adoptadas para minimizar el riesgo de da±o hepßtico. [On line] | Link |Crist¾bal Garcia I, Goitia Ibarra M, Raga Baixauli F. Acetato de ulipristal despuķs del proceso de la Agencia Europea del Medicamento. ┐Quķ ha sucedido y cußl es la visi¾n actual?. Prog Obstet Ginecol 2018;61(6):535-539. | Link |Neha Shah, Elizabeth Egbase, Michail Sideris, Samuel Oxley, Funlayo Odejinmi. The treatment of uterine fibroids with ulipristal acetate: a systematic review of real-world data. PROSPERO 2019 CRD42019151393. Jin Ximeng, Fan Dongmei. Acetato de ulipristal para fibromas uterinos: una revisi¾n sistemßtica y metanßlisis. PROSPERO 2015 CRD42015019778. Margarete Bristot. Ulipristal acetate: medical therapy for uterine fibroids. PROSPERO 2015 CRD42015024333 Sangam Jha. Ulipristal acetate in the management of fibroid uterus. Dang Q Vinh. Ulipristal Acetate in Symptomatic Uterine Fibroid. 






 Estudios originales
Estudios originales