Revista Biomédica Revisada Por Pares

 Para Descargar PDF debe Abrir sesión.
Para Descargar PDF debe Abrir sesión.
Palabras clave: Age-related macular degeneration, treat and extend, pro re nata, neovascular, Epistemonikos, GRADE.
INTRODUCTION
Age-related macular degeneration is the leading cause of blindness in older people in the world. One of the most effective treat-ments consists of injection intravitreal of anti-endothelial vascular growth factor (anti-VEGF) drugs. However, there is no con-sensus on their frequency of administration, being the treat and extend and the pro re nata the most commonly used regimens, but there is still controversy regarding their effectiveness.
METHODS
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS
We identified two systematic reviews that together included two primary studies, both observational studies. We concluded that we are uncertain whether the treat and extend regimen is superior in terms of visual gain, decrease in retinal thickness, number of injections and serious adverse effects at 12 months in comparison with the pro re nata regimen, because the certainty of the existing evidence has been assessed as very low.
Age-related macular degeneration is the leading cause of blindness in people over 50 years of age [1] and its global projection is estimated to reach 288 million cases in 2040 [2]. The disease is a result of the excessive accumulation of drusen, a residual material that can be found in the macula or peripheral retina, which produces the histological changes leading to macular degeneration [1].
Currently, one of the most effective treatments for neovascular age-related macular degeneration of injection of drugs against endothelial vascular growth factor [3] (anti-VEGF), but there is no consensus in the literature on the frequency of administrations, or under which specific criteria the injections should be applied.
Among its application protocols, we can find the fixed regimes that generally consist of monthly injections, the pro re nata consisting of monthly visits and administration of medication only if there are certain findings on the ophthalmological examination, and thirdly the treat and extend regimen, in which the drug is supplied independent of what is observed by the specialist, but the visit intervals are defined according to the examination, which can range from four to twelve weeks [4].
In this summary, we aimed to evaluate the effectiveness and safety of the treat and extend regimen in comparison with the pro re nata regimen, whose use is still controversial.
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
|
What is the evidence. |
We identified two systematic reviews [5], [6], that included two observational studies [7], [8]. |
|
What types of patients were included* |
Both studies included patients with the diagnosis of neovascular age-related macular degeneration, regardless of stage. One study included patients treated between 2007 and 2008 [7], and one between 2010 and 2014 [8]. One study included only Caucasians with visual acuity over 0.5 (Snellen) [8]. |
|
What types of interventions were included* |
The two studies evaluated treatment with anti-VEGF drugs, comparing treat and extend versus pro re nata regimens [7], [8]. In both studies ranibizumab was used as the anti-VEGF drug in doses of 0.5 milligrams per injection [7], [8]. |
|
What types of outcomes |
The studies reported multiple outcomes, which were grouped by the systematic reviews as follows:
|
* Information about primary studies is not extracted directly from primary studies but from identified systematic reviews, unless otherwise stated.
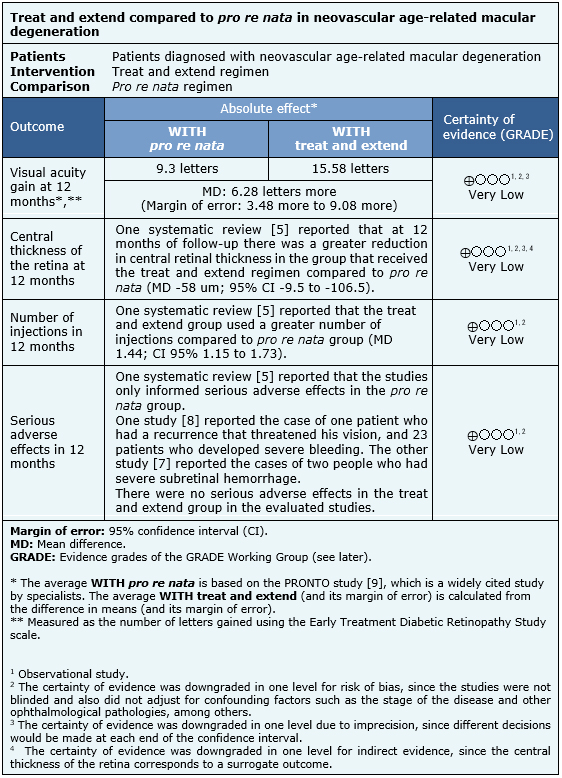
The information presented on the effects of the use of treat and extend versus pro re nata is based on two observational studies that included 230 patients [5], [6].
The two observational studies measured visual acuity gain at 12 months, serious adverse effects in 12 months and the number of injections in 12 months in each regimen [7], [8] [230 patients]. One study also measured the central thickness of the retina at 12 months (140 patients) [8].
However, no systematic review allowed data extraction of central thickness of the retina, number of injections and serious adverse effects in a way that they could be incorporated into a meta-analysis, so the information of these outcomes is presented as a narrative synthesis of the only review that identified both studies [5].
The summary of findings is as follows:
| Follow the link to access the interactive version of this table (Interactive Summary of Findings – iSoF) |

|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
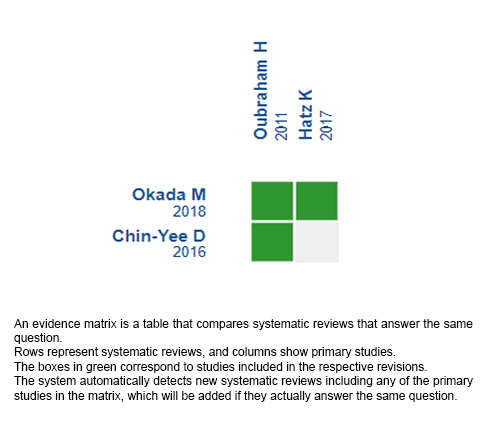
Follow the link to access the interactive version: Treat and extend versus pro re nata in age-related macular degeneration.
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
 Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
INTRODUCTION
Age-related macular degeneration is the leading cause of blindness in older people in the world. One of the most effective treat-ments consists of injection intravitreal of anti-endothelial vascular growth factor (anti-VEGF) drugs. However, there is no con-sensus on their frequency of administration, being the treat and extend and the pro re nata the most commonly used regimens, but there is still controversy regarding their effectiveness.
METHODS
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS
We identified two systematic reviews that together included two primary studies, both observational studies. We concluded that we are uncertain whether the treat and extend regimen is superior in terms of visual gain, decrease in retinal thickness, number of injections and serious adverse effects at 12 months in comparison with the pro re nata regimen, because the certainty of the existing evidence has been assessed as very low.
Autor:
Rodolfo Garretón[1,2], Raúl González[1,2]
Citación: Garretón R, González R. Treat and extend compared to pro re nata regimen in neovascular age-related macular degeneration. Medwave 2020;20(08):e8023 doi: 10.5867/medwave.2020.08.8023
Fecha de publicación: 11/9/2020
Origen: Este artículo es producto del Epistemonikos Evidence Synthesis Project de la Fundación Epistemonikos, en colaboración con Medwave para su publicación.
Tipo de revisión: Con revisión por pares sin ciego por parte del equipo metodológico del Centro Evidencia UC en colaboración con Epistemonikos Evidence Synthesis Project.
Nos complace que usted tenga interés en comentar uno de nuestros artículos. Su comentario será publicado inmediatamente. No obstante, Medwave se reserva el derecho a eliminarlo posteriormente si la dirección editorial considera que su comentario es: ofensivo en algún sentido, irrelevante, trivial, contiene errores de lenguaje, contiene arengas políticas, obedece a fines comerciales, contiene datos de alguna persona en particular, o sugiere cambios en el manejo de pacientes que no hayan sido publicados previamente en alguna revista con revisión por pares.
Aún no hay comentarios en este artículo.
Para comentar debe iniciar sesión
Medwave publica las vistas HTML y descargas PDF por artículo, junto con otras métricas de redes sociales.
Jager R, Mieler W, Miller J. Age-Related Macular Degeneration. New England Journal of Medicine. 2008;358(24):2606-2617. Wong WL, Su X, Li X, Cheung CM, Klein R, Cheng CY, Wong TY. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014 Feb;2(2):e106-16. | CrossRef | PubMed |Lim L, Mitchell P, Seddon J, Holz F, Wong T. Age-related macular degeneration. The Lancet. 2012;379(9827):1728-1738. Kim L, Mehta H, Barthelmes D, Nguyen V, Gillies M. METAANALYSIS OF REAL-WORLD OUTCOMES OF INTRAVITREAL RANIBIZUMAB FOR THE TREATMENT OF NEOVASCULAR AGE-RELATED MACULAR DEGENERATION. Retina. 2016;36(8):1418-1431. Okada M, Kandasamy R, Chong E, McGuiness M, Guymer R. The Treat-and-Extend Injection Regimen Versus Alternate Dosing Strategies in Age-related Macular Degeneration: A Systematic Review and Meta-analysis. American Journal of Ophthalmology. 2018;192:184-197. Chin-Yee D, Eck T, Fowler S, Hardi A, Apte R. A systematic review of as needed versus treat and extend ranibizumab or bevacizumab treatment regimens for neovascular age-related macular degeneration. British Journal of Ophthalmology. 2015;100(7):914-917. Oubraham H, Cohen S, Samimi S, Marotte D, Bouzaher I, Bonicel P et al. INJECT AND EXTEND DOSING VERSUS DOSING AS NEEDED. Retina. 2011;31(1):26-30. Hatz K, Prünte C. Treat and Extend versus Pro Re Nata regimens of ranibizumab in neovascular age-related macular degeneration: a comparative 12 Month study. Acta Ophthalmologica. 2016;95(1):e67-e72. Fung A, Lalwani G, Rosenfeld P, Dubovy S, Michels S, Feuer W et al. An Optical Coherence Tomography-Guided, Variable Dosing Regimen with Intravitreal Ranibizumab (Lucentis) for Neovascular Age-related Macular Degeneration. American Journal of Ophthalmology. 2007;143(4):566-583.e2. “Tratamiento de la Degeneración Macular Asociada a la Edad (DMAE) Exudativa y Atrófica. Guías de Práctica Clínica de la SERV”. | Link |American Academy of Ophtalmology Retina/Vitreous Panel. Preferred Practice Pattern® Guidelines. Age-Related Macular Degeneration. San Francisco, Ca: American Academy of Ophtalmology; 2015. | Link |






 Estudios originales
Estudios originales