Revista Biomédica Revisada Por Pares

 Para Descargar PDF debe Abrir sesión.
Para Descargar PDF debe Abrir sesión.
Palabras clave: knee osteoarthritis, cane, Epistemonikos, GRADE
Introduction
Knee osteoarthritis is a relevant health problem given its high prevalence and associated disability. Within the non-pharmacological management alternatives, the use of canes has been proposed, however, there is no consensus in the literature regarding its indication.
Methods
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
Results and conclusions
We identified three systematic reviews including four studies overall, of which one was randomized trials. We conclude that the use of a contralateral cane in patients with knee osteoarthritis probably reduces pain. In addition, it could slightly increase function, but the certainty of the evidence is low.
Osteoarthritis is a relevant health problem, with hip and knee osteoarthritis the eleventh leading cause of global disability, the thirty-eighth in years of life adjusted for disability[1] and an important reason for consultation in both primary and specialist care. Conservative management is the first line of treatment and its main objective is pain control. This includes the use of drugs, patient education, weight loss in patients with obesity, kinesiotherapy and the use of technical aids such as the cane, among others. The cane is used with the aim of reducing the biomechanical load that is exerted on the hip and knee. However, there is no consensus in the literature about its effect or its indication.
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
|
What is the evidence See evidence matrix in Epistemonikos later |
We found three systematic reviews[2],[3],[4], which included four primary studies[5],[6],[7],[8] of which one corresponds to a randomized trial[7]. All the studies reported interesting outcomes, for which reason this table and the summary, in general, are based on these. |
|
What types of patients were included* |
All the studies[5],[6],[7],[8] included adult patients with a diagnosis of knee osteoarthritis, based on the American College of Rheumatology criteria, all of which presented symptoms (pain). The average age ranged from 53.6 to 65 years. 76.5% of the patients were women. |
|
What types of interventions were included* |
One study[5] evaluated the use of a contralateral walking pole, one trial[7] analyzed the use of a wooden cane with a contralateral T-shaped handle, the other two studies[6],[8] used contralateral cane not specifying the type. Three studies[5],[6], [8] compared the same patients without the use of canes, while one trial[7] compared a control group with knee osteoarthritis. |
|
What types of outcomes were measured |
Of the multiple outcomes measured by the trials, the systematic reviews presented in a grouped manner the following: pain, function, quality of life, walking speed, moment of adduction of the knee and vertical reaction force to the ground. The average follow-up of the trials was one month (range between 0 and 2 months). |
* Information about primary studies is not extracted directly from primary studies but from identified systematic reviews, unless otherwise stated.
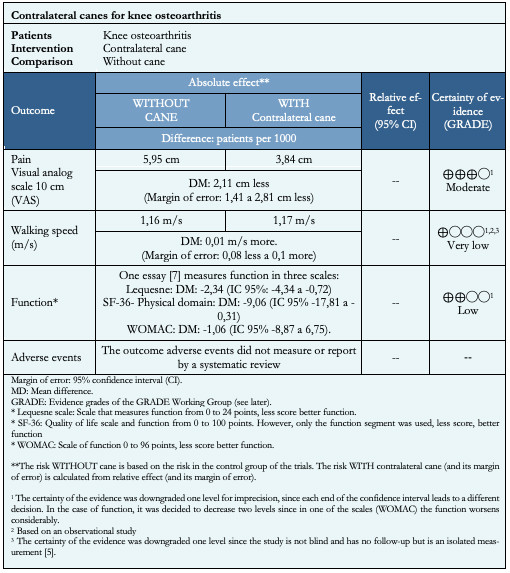
The information on the effects of the use of canes in knee osteoarthritis is based on two studies, one observational[5] and one randomized[7], which included 98 patients.
The randomized trial[7] measured pain and function outcomes (64 patients), while the observational study[5] measured the walking speed outcome (34 patients).
The summary of the results is as follows:
The use of contralateral cane in patients with knee osteoarthritis probably decreases the pain (certainty of the evidence is moderate).
It is not possible to establish clearly if contralateral cane use increases walking speed, because the certainty of the existing evidence has been evaluated as very low.
The use of a contralateral cane could slightly increase function (certainty of the evidence is low).
| Follow the link to access the interactive version of this table (Interactive Summary of Findings – iSoF) |

|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
| Differences between this summary and others sources |
|
| Could this evidence change in the future? |
|
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
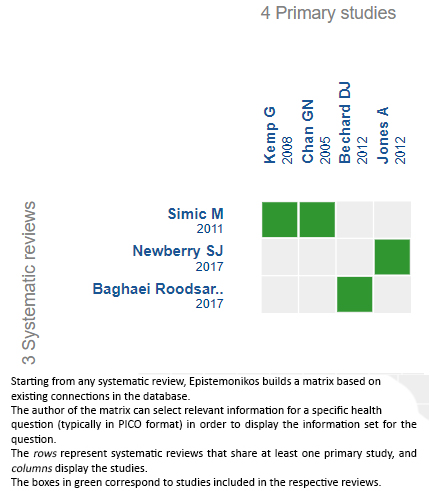
| Follow the link to access the interactive version: Canes for knee osteoarthritis |
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwaveor to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
 Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
Introduction
Knee osteoarthritis is a relevant health problem given its high prevalence and associated disability. Within the non-pharmacological management alternatives, the use of canes has been proposed, however, there is no consensus in the literature regarding its indication.
Methods
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
Results and conclusions
We identified three systematic reviews including four studies overall, of which one was randomized trials. We conclude that the use of a contralateral cane in patients with knee osteoarthritis probably reduces pain. In addition, it could slightly increase function, but the certainty of the evidence is low.
Autores:
Francesca Moller[1,2], Luis Ortiz-Muńoz[2,3], Sebastián Irarrázaval[2,4]
Citación: Moller F, Ortiz-Muńoz L, Irarrázaval S. Contralateral canes for knee osteoarthritis. Medwave 2020;20(1):e7759 doi: 10.5867/medwave.2020.01.7759
Fecha de envío: 11/3/2019
Fecha de aceptación: 17/5/2019
Fecha de publicación: 16/1/2020
Origen: Este artículo es producto del Epistemonikos Evidence Synthesis Project de la Fundación Epistemonikos, en colaboración con Medwave para su publicación
Tipo de revisión: Con revisión por pares sin ciego por parte del equipo metodológico del Epistemonikos Evidence Synthesis Project
Nos complace que usted tenga interés en comentar uno de nuestros artículos. Su comentario será publicado inmediatamente. No obstante, Medwave se reserva el derecho a eliminarlo posteriormente si la dirección editorial considera que su comentario es: ofensivo en algún sentido, irrelevante, trivial, contiene errores de lenguaje, contiene arengas políticas, obedece a fines comerciales, contiene datos de alguna persona en particular, o sugiere cambios en el manejo de pacientes que no hayan sido publicados previamente en alguna revista con revisión por pares.
Aún no hay comentarios en este artículo.
Para comentar debe iniciar sesión
Medwave publica las vistas HTML y descargas PDF por artículo, junto con otras métricas de redes sociales.
Cross M, Smith E, Hoy D, Nolte S, Ackerman I, Fransen M, et al. The global burden of hip and knee osteoarthritis: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014 Jul;73(7):1323-30. | CrossRef | PubMed |Baghaei Roodsari R, Esteki A, Aminian G, Ebrahimi I, Mousavi ME, Majdoleslami
B, et al. The effect of orthotic devices on knee adduction moment, pain and
function in medial compartment knee osteoarthritis: a literature review. Disabil
Rehabil Assist Technol. 2017 Jul;12(5):441-449. | CrossRef | PubMed |Newberry SJ, FitzGerald J, SooHoo NF, Booth M, Marks J, Motala A, et al. Treatment of Osteoarthritis of the Knee:
An Update Review. Rockville (MD): Agency for Healthcare Research and
Quality (US); 2017 May. [on line] | PubMed | Link |Simic M, Hinman RS, Wrigley TV, Bennell KL, Hunt MA. Gait modification strategies for altering medial knee joint load: a systematic review. Arthritis Care Res (Hoboken). 2011 Mar;63(3):405-26. | CrossRef | PubMed |Bechard DJ, Birmingham TB, Zecevic AA, Jones IC, Leitch KM, Giffin JR, et al. The effect of walking poles on the knee adduction moment in patients with varus gonarthrosis. Osteoarthritis Cartilage. 2012 Dec;20(12):1500-6. | CrossRef | PubMed |Chan GN, Smith AW, Kirtley C, Tsang WW. Changes in knee moments with
contralateral versus ipsilateral cane usage in females with knee osteoarthritis.
Clin Biomech (Bristol, Avon). 2005 May;20(4):396-404. | PubMed |Jones A, Silva PG, Silva AC, Colucci M, Tuffanin A, Jardim JR, et al. Impact of cane use on pain, function, general health and energy expenditure
during gait in patients with knee osteoarthritis: a randomised controlled trial.
Ann Rheum Dis. 2012 Feb;71(2):172-9. | CrossRef | PubMed |Kemp G, Crossley KM, Wrigley TV, Metcalf BR, Hinman RS. Reducing joint loading
in medial knee osteoarthritis: shoes and canes. Arthritis Rheum. 2008 May
15;59(5):609-14. | CrossRef | PubMed |Hart J, Hinman RS, van Ginckel A, Hall M, Nelligan R, Bennell KL. Factors
Influencing Cane Use for the Management of Knee Osteoarthritis: A Cross-Sectional
Survey. Arthritis Care Res (Hoboken). 2018 Oct;70(10):1455-1460. | CrossRef | PubMed |Guyatt GH, Oxman AD, Kunz R, Atkins D, Brozek J, Vist G, et al. GRADE guidelines: 2. Framing the question and
deciding on important outcomes. J Clin Epidemiol. 2011 Apr;64(4):395-400. | CrossRef | PubMed |McAlindon TE, Bannuru RR, Sullivan MC, Arden NK, Berenbaum F, Bierma-Zeinstra
SM, et al. OARSI guidelines for the non-surgical management of knee
osteoarthritis. Osteoarthritis Cartilage. 2014 Mar;22(3):363-88. | CrossRef | PubMed |Brown GA. AAOS clinical practice guideline: treatment of osteoarthritis of
the knee: evidence-based guideline, 2nd edition. J Am Acad Orthop Surg. 2013
Sep;21(9):577-9. | CrossRef | PubMed |Bowd J, Biggs P, Whatling G, Holt C. Do gait style and gait retraining have the potential to reduce medial compartmental loading in individuals with knee osteoarthritis whilst not adversely affecting the hip and ankle joints? Protocol for a systematic review. PROSPERO 2018 CRD42018085738 [on line] | Link |Fang M. Walking Aids in the Management of Knee Osteoarthritis. ClinicalTrials.gox. [on line] | Link |Jones A. Effectiveness of Cane in Osteoarthritis (OA) Patients. ClinicalTrials.gox. [on line] | Link |






 Estudios originales
Estudios originales