Revista Biomédica Revisada Por Pares

 Para Descargar PDF debe Abrir sesión.
Para Descargar PDF debe Abrir sesión.
Palabras clave: caries removal, minimally invasive dentistry, Epistemonikos, GRADE
INTRODUCTION
Dental caries have been conventionally managed by non-selective removal of carious tissue (total complete removal); however, the adverse effects of this procedure have promoted the use of conservative caries removal techniques (selective removal), but there is still controversy regarding its effectiveness.
METHODS
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS
We identified seven systematic reviews including seven studies overall, of which all were randomized trials. We concluded that selective caries removal may decrease the need for root canal treatment and the risk of pulp exposure in teeth with deep caries, but the certainty of the evidence is low. It is not clear whether the selective removal of caries reduces the risk of appearance of signs and symptoms of pulp disease and the risk of restorations failure, as the certainty of the evidence is very low.
Dental caries is the most prevalent dental disease worldwide[1]. Traditionally, its treatment involves non-selective (complete) removal of carious and demineralized tissue, and subsequent restoration of the dental piecetooth[2]. However, this dental preparation technique has been questioned in recent years for the associated adverse effects, such as pulp exposure and development of pulp disease[2],[3].
Consequently, conservative techniques have emerged as an alternative for the treatment of deep caries. One of them consists of the selective removal of carious tissue, in order to preserve as much dental structure as possible and so avoiding adverse effects[4]. This technique has been defined in various ways in the literature, with discrepancies in excavation depth and clinical removal criteria. The most accepted definition is the one proposed by the International Caries Consensus Collaboration (ICCC), which defines selective removal as the excavation technique in which peripheral dentin is removed until only hard dentin is left, while the pulp wall is excavated until reaching firm or soft dentine[5].
However, it has been suggested that this technique would lead to restoration failures, so its use remains controversial[6]. This summary aims to evaluate the effectiveness and safety of selective caries removal compared to complete removal.
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
|
What is the evidence See evidence matrix in Epistemonikos later |
We found seven systematic reviews[4],[7],[8],[9],[10],[11],[12] which included seven primary studies overall, reported in nine references[13],[14],[15],[16],[17],[18],[19],[20],[21], all of which correspond to randomized trials. |
|
What types of patients were included* |
Of the seven trials, five included only children (3 to 11 years old)[13],[14],[15],[18],[20] and two included children and adolescents (4 to 17 years old) [17],[19]. Four included only temporary teeth[13],[14],[17],[19], one trial included only permanent teeth[19], and two both dentitions[13],[17]. Regarding the extent of caries, all trials included only deep tooth decay, excluding those lesions circumscribed only to enamel. Five trials included occlusal and proximal caries[13],[14],[17],[18],[20], while two included only occlusal caries[15],[19]. Finally, all trials excluded patients with irreversible pulp symptoms and/or apical lesion prior to inclusion[13],[14],[15],[17],[18],[19],[20]. |
|
What types of interventions were included* |
All trials compared the selective removal of deep dental caries against conventional treatment (complete removal). Selective removal was described in various ways by the different trials, but in general it was defined as the excavation of the remaining dentin from the floor of the cavity near the pulp, soft to the touch, of sticky consistency and soft to the probing procedure[8]. None of the reviews included information on the instruments used or the depth of excavation. |
|
What types of outcomes were measured |
The trials measured multiple outcomes, which were pooled by the systematic reviews as follows:
The follow-up ranged between 6[15],[17],[18],[20] and 24 months[13],[14],[19]. |
* Information about primary studies is not extracted directly from primary studies but from identified systematic reviews, unless otherwise stated.
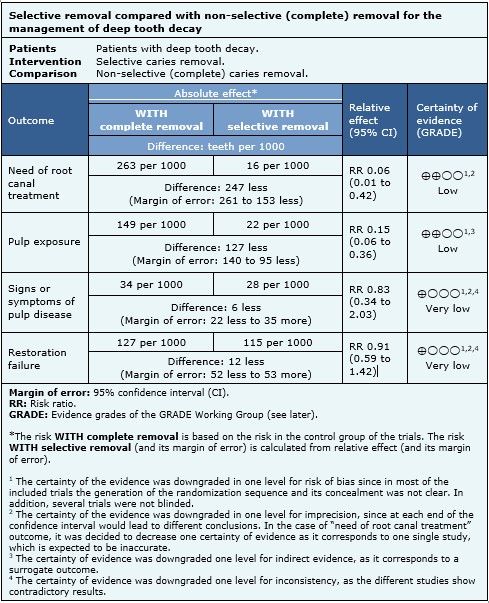
The information on the effects of selective caries removal is based on seven randomized trials that included 570 patients.
Regarding safety-related outcomes, only one trial reported the events needing root canal treatment (48 patients, 120 teeth)[14], four trials reported the events of pulp exposure (477 patients, 489 teeth) [14],[15],[17],[18] and six analyzed the signs or symptoms of pulp disease (526 patients, 555 teeth)[14],[15],[17],[18],[19],[20]. With regard to effectiveness, all trials evaluated the events of restoration failure (570 patients, 641 teeth)[13],[14],[15],[17],[18],[19],[20].
The summary of findings is as follows:
Selective caries removal may decrease the need for root canal treatment in teeth with deep caries (low certainty of the evidence).
Selective caries removal may decrease the risk of pulp exposure in teeth with deep caries (low certainty of the evidence).
We are uncertain whether selective caries removal decreases the risk of the appearance of signs and symptoms of pulp disease as the certainty of the evidence has been assessed as very low.
We are uncertain whether selective caries removal decreases the risk of restoration failure as the certainty of the evidence has been assessed as very low.
|
Follow the link to access the interactive version of this table (Interactive Summary of Findings – iSoF) |

|
To whom this evidence does and does not apply |
|
|
About the outcomes included in this summary |
|
|
Balance between benefits and risks, and certainty of the evidence |
|
|
Resource considerations |
|
|
What would patients and their doctors think about this intervention |
|
|
Differences between this summary and others sources |
|
|
Could this evidence change in the future? |
|
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
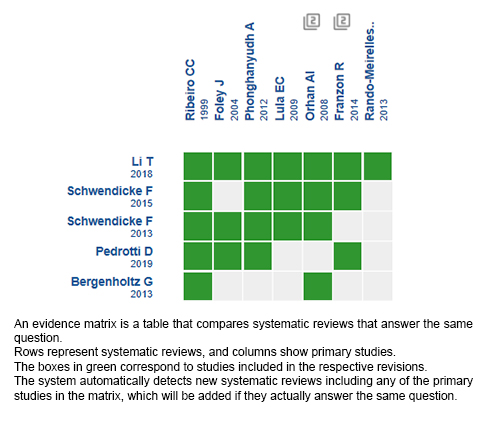
Follow the link to access the interactive version: Selective removal versus complete removal of deep caries lesions
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
 Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
INTRODUCTION
Dental caries have been conventionally managed by non-selective removal of carious tissue (total complete removal); however, the adverse effects of this procedure have promoted the use of conservative caries removal techniques (selective removal), but there is still controversy regarding its effectiveness.
METHODS
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS
We identified seven systematic reviews including seven studies overall, of which all were randomized trials. We concluded that selective caries removal may decrease the need for root canal treatment and the risk of pulp exposure in teeth with deep caries, but the certainty of the evidence is low. It is not clear whether the selective removal of caries reduces the risk of appearance of signs and symptoms of pulp disease and the risk of restorations failure, as the certainty of the evidence is very low.
Autores:
Francisca Verdugo-Paiva[1,3], Paula Zambrano-Achig[2,3], Daniel Simancas-Racines[2,3], Andrés Viteri-García[2,3]
Citación: Verdugo-Paiva F, Zambrano-Achig P, Simancas-Racines D, Viteri-García A. Selective removal compared to complete removal for deep carious lesions. Medwave 2020;20(1):e7758 doi: 10.5867/medwave.2020.01.7758
Fecha de envío: 14/5/2019
Fecha de aceptación: 28/11/2019
Fecha de publicación: 28/1/2020
Origen: Este artículo es producto del Epistemonikos Evidence Synthesis Project de la Fundación Epistemonikos, en colaboración con Medwave para su publicación
Tipo de revisión: Con revisión por pares sin ciego por parte del equipo metodológico del Epistemonikos Evidence Synthesis Project
Nos complace que usted tenga interés en comentar uno de nuestros artículos. Su comentario será publicado inmediatamente. No obstante, Medwave se reserva el derecho a eliminarlo posteriormente si la dirección editorial considera que su comentario es: ofensivo en algún sentido, irrelevante, trivial, contiene errores de lenguaje, contiene arengas políticas, obedece a fines comerciales, contiene datos de alguna persona en particular, o sugiere cambios en el manejo de pacientes que no hayan sido publicados previamente en alguna revista con revisión por pares.
Aún no hay comentarios en este artículo.
Para comentar debe iniciar sesión
Medwave publica las vistas HTML y descargas PDF por artículo, junto con otras métricas de redes sociales.
Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005 Sep;83(9):661-9. | PubMed |White JM, Eakle WS. Rationale and treatment approach in minimally invasive dentistry. J Am Dent Assoc. 2000 Jun;131 Suppl:13S-19S. | PubMed |Banerjee A. Minimal intervention dentistry: part 7. Minimally invasive operative caries management: rationale and techniques. Br Dent J. 2013 Feb;214(3):107-11. | CrossRef | PubMed |Schwendicke F, Frencken JE, Bjřrndal L, Maltz M, Manton DJ, Ricketts D, et al. Managing Carious Lesions: Consensus Recommendations on Carious Tissue Removal. Adv Dent es. 2016 May;28(2):58-67. | CrossRef | PubMed |Schwendicke F, Göstemeyer G. Understanding dentists' management of deep carious lesions in permanent teeth: a systematic review and meta-analysis. Implement Sci. 2016 Oct 19;11(1):142. | PubMed |Li T, Zhai X, Song F, Zhu H. Selective versus non-selective removal for dental caries: a systematic review and meta-analysis. Acta Odontol Scand. 2018 Mar;76(2):135-140. | CrossRef | PubMed |Bergenholtz G, Axelsson S, Davidson T, Frisk F, Hakeberg M, Kvist T, et al. Treatment of pulps in teeth affected by deep caries - A systematic review of the literature. Singapore Dent J. 2013 Dec;34(1):1-12. | CrossRef | PubMed |Schwendicke F, Paris S, Tu YK. Effects of using different criteria for caries removal: a systematic review and network meta-analysis. J Dent. 2015 Jan;43(1):1-15. | CrossRef | PubMed |Schwendicke F, Dörfer CE, Paris S. Incomplete caries removal: a systematic review and meta-analysis. J Dent Res. 2013 Apr;92(4):306-14. | CrossRef | PubMed |Thompson V, Craig RG, Curro FA, Green WS, Ship JA. Treatment of deep carious lesions by complete excavation or partial removal: a critical review. J Am Dent Assoc. 2008 Jun;139(6):705-12. | PubMed |Ferreira JM, Pinheiro SL, Sampaio FC, de Menezes VA. Caries removal in primary teeth--a systematic review. Quintessence Int. 2012 Jan;43(1):e9-15. | PubMed |Pedrotti D, Cavalheiro CP, Casagrande L, de Araújo FB, Pettorossi Imparato JC, de Oliveira Rocha R, et al. Does selective carious tissue removal of soft dentin increase the restorative failure risk in primary teeth?: Systematic review and meta-analysis. J Am Dent Assoc. 2019 Jul;150(7):582-590.e1. | CrossRef | PubMed |Foley J, Evans D, Blackwell A. Partial caries removal and cariostatic materials in carious primary molar teeth: a randomised controlled clinical trial. Br Dent J. 2004 Dec 11;197(11):697-701; discussion 689. | PubMed |Franzon R, Guimarăes LF, Magalhăes CE, Haas AN, Araujo FB. Outcomes of one-step incomplete and complete excavation in primary teeth: a 24-month randomized controlled trial. Caries Res. 2014;48(5):376-83. | CrossRef | PubMed |Lula EC, Monteiro-Neto V, Alves CM, Ribeiro CC. Microbiological analysis after complete or partial removal of carious dentin in primary teeth: a randomized clinical trial. Caries Res. 2009;43(5):354-8. | CrossRef | PubMed |Orhan AI, Oz FT, Ozcelik B, Orhan K. A clinical and microbiological comparative study of deep carious lesion treatment in deciduous and young permanent molars. Clin Oral Investig. 2008 Dec;12(4):369-78. | CrossRef | PubMed |Orhan AI, Oz FT, Orhan K. Pulp exposure occurrence and outcomes after 1- or 2-visit indirect pulp therapy vs complete caries removal in primary and permanent molars. Pediatr Dent. 2010 Jul-Aug;32(4):347-55. | PubMed |Phonghanyudh A, Phantumvanit P, Songpaisan Y, Petersen PE. Clinical evaluation of three caries removal approaches in primary teeth: a randomised controlled trial. Community Dent Health. 2012 Jun;29(2):173-8. | PubMed |Rando-Meirelles MPM, Tôrres LHN, Sousa MLR. Twenty-Four Months Of Follow-Up After Partial Removal Of Carious Dentin: A Preliminary Study. Dentistry. 2013; (3):162. | CrossRef |Ribeiro CC, Baratieri LN, Perdigăo J, Baratieri NM, Ritter AV. A clinical, radiographic, and scanning electron microscopic evaluation of adhesive restorations on carious dentin in primary teeth. Quintessence Int. 1999 Sep;30(9):591-9. | PubMed |Franzon R, Opdam NJ, Guimarăes LF, Demarco FF, Casagrande L, Haas AN, et al. Randomized controlled clinical trial of the 24-months survival of composite resin restorations after one-step incomplete and complete excavation on primary teeth. J Dent. 2015 Oct;43(10):1235-41. | CrossRef | PubMed |Schwendicke F, Mostajaboldave R, Otto I, Dörfer CE, Burkert S. Patients' preferences for selective versus complete excavation: A mixed-methods study. J Dent. 2016 Mar;46:47-53. | CrossRef | PubMed |American Academy of Pediatric Dentistry (AAPD). Guideline on Restorative Dentistry. Reference Manual. 2015; 37(6): 232-43. ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). Identifier NCT02286388., Multicenter Trial Comparing One-step Partial Caries Removal to Complete Caries Removal for the Treatment of Deep Carious Lesions in Permanent Teeth. (DECAT : DEep CAries Treatment). (DECAT); 2014 Nov 7. [On line]. | Link |






 Estudios originales
Estudios originales