Revista BiomÈdica Revisada Por Pares

 Para Descargar PDF debe Abrir sesiÛn.
Para Descargar PDF debe Abrir sesiÛn.
Este texto completo es la transcripciÛn editada y revisada de una conferencia dictada en las Jornadas Latinoamericanas de C·ncer de Mama 2002, organizadas por la Escuela Latinoamericana de MastologÌa, FederaciÛn Latinoamericana de MastologÌa y Sociedad Chilena de MastologÌa.
Editor CientÌfico: Dr. Hernando Paredes.
En las ˙ltimas dÈcadas se ha obtenido un considerable progreso en el tratamiento del c·ncer de mama. Los dos aspectos m·s relevantes en este avance han sido los siguientes:
La selecciÛn del tratamiento adyuvante para el carcinoma de mama en estadÌos poco avanzados se basa en los Factores PronÛsticos y Predictivos.
Los factores pronÛsticos son medidas o determinaciones disponibles en el momento del diagnÛstico lo que, en ausencia de un tratamiento adyuvante sistÈmico, se asocia con una mayor frecuencia de recidivas y recurrencias tumorales asÌ como con una mayor mortalidad. Los factores pronÛsticos ayudan a predecir la historia natural del tumor.
Los factores predictivos son mediciones que se asocian con la respuesta o ausencia de respuesta a un tratamiento especÌfico.
Los factores pronÛsticos (1,2,3) habitualmente utilizados para seleccionar el tratamiento adyuvante sistÈmico en el carcinoma de mama son:
El tamaÒo tumoral es un predictor significativo de la recurrencia del carcinoma de mama. C·lculos del San Antonio Data Base seÒalan que el riesgo de recurrencia en el c·ncer de mama con ganglios negativos aumenta con el tamaÒo tumoral creciente (5). El estudio comparativo del tamaÒo tumoral con otras variables, tales como grado histolÛgico, p53, c-erb-B2, receptores de estrÛgenos y receptores de progesterona, ratificÛ el valor que el tamaÒo del tumor tiene por sÌ solo (6,7).
Los grados histolÛgico y nuclear constituyen un factor pronÛstico independiente en el c·ncer de mama con ganglios negativos. La objeciÛn que se les hace es que el sistema que establece los grados es, generalmente, subjetivo, con un factor limitante que es la ausencia de reproducibilidad y variabilidad entre los observadores.
Diversos factores expresan la proliferaciÛn celular y se pueden emplear para medir directamente la proliferaciÛn de las cÈlulas tumorales. Ellos son Ki 67 (anticuerpo monoclonal especÌfico para un antÌgeno nuclear expresado en cÈlulas proliferentes), Ìndice mitÛtico, fracciÛn de fase S (por citometrÌa de flujo) y el Ìndice de marcaciÛn con timidina (8). La incorporaciÛn de timidina es un factor predictivo de la utilidad de la quimioterapia adyuvante; se ha comprobado una mayor sobrevida libre de enfermedad en pacientes tratadas con quimioterapia, quienes tenÌan tumores con alto Ìndice proliferativo (13,14).
El estado menop·usico predice para la respuesta terapÈutica a la ooforectomÌa (9). TambiÈn el estado menop·usico predice para la eficacia de la quimioterapia adyuvante, pero no predice para la eficacia del tamoxifeno. El estado menop·usico se correlaciona, habitualmente, con el estado del receptor hormonal, pero ello no significa que permita presumir su positividad para seleccionar el tratamiento adyuvante sistÈmico.
De los nuevos marcadores biolÛgicos y moleculares no existen a˙n estudios definitivos. Persisten dificultades tÈcnicas que impiden validar el significado pronÛstico de p53 y de cuantificar la pÈrdida de la funciÛn apoptÛtica celular (6,11,12).
En relaciÛn al valor de Her2neu como factor pronÛstico, un metaan·lisis reciente no logrÛ avalar su uso como factor pronÛstico puro (15). Hayes et al. (16) seÒalan que en pacientes no tratados, HER 2 tiene un valor, como factor pronÛstico, entre dÈbil y moderadamente fuerte. Adem·s de ser HER 2 un blanco para tratamiento especÌfico, es probablemente un predictor de respuesta a la quimioterapia y hormonoterapia. La sobreexpresiÛn o amplificaciÛn de HER 2 se traduce en un menor beneficio con el uso de tamoxifeno adyuvante (16,17). Asimismo, los tumores que sobreexpresan HER 2 tienen mayor sensibilidad a la quimioterapia adyuvante con esquemas que contengan antraciclÌnicos (18). Andrulis et al. (19) han seÒalado que la amplificaciÛn de HER 2 en c·ncer de mama con ganglios negativos es un factor pronÛstico adverso e independiente para el riesgo de recurrencia.
La extensiÛn de la microvascularizaciÛn tumoral es un factor determinante para el desarrollo de posibles micromet·stasis. Se han podido identificar marcadores anticipados de la invasiÛn microvascular. Dentro de Èstos tenemos el factor de crecimiento del endotelio vascular (VEGF), el activador del plasminÛgeno tipo urokinasa (uPA) y el activador del inhibidor tipo I del plasminÛgeno (PAI-1). Adem·s de lo seÒalado previamente, la medida de la invasiÛn linf·tica y vascular a nivel del tumor aporta informaciÛn pronÛstica significativa, tal como se seÒalÛ aÒos atr·s (20). El VEFG tiene un impacto pronÛstico propio, que se puede incrementar significativamente combin·ndolo con uPA (21). La uPA, proteasa del tejido tumoral, y su inhibidor PAI-1 son marcadores biolÛgicos asociados a las cÈlulas tumorales, que participan en el proceso de invasiÛn, migraciÛn celular, adhesiÛn, angiogÈnesis y producciÛn de met·stasis. Ambas molÈculas son poderosos factores pronÛsticos independientes de recurrencia tumoral y de muerte, en portadoras de c·ncer de mama con ganglios negativos o positivos (22,23,24). Thomssen, en Alemania (25), evaluÛ prospectivamente ambos marcadores y seÒalÛ que el grado tumoral y uPA/PAI-1 son los factores pronÛsticos independientes m·s significativos en pacientes no tratadas con c·ncer de mama con ganglios negativos.
La detecciÛn de micromet·stasis ganglionares o en la mÈdula Ûsea puede llegar a constituirse en otro factor de relevancia. En pacientes con ganglios negativos por microscopÌa convencional se han comprobado micromet·stasis hasta en 10% a 20% de los casos, seg˙n diferentes series. Para convalidarlas se esperan resultados definitivos que surjan de ensayos prospectivos. Por su parte, la detecciÛn de micromet·stasis en la mÈdula Ûsea mantiene a˙n dudas conceptuales sobre si constituye o no un factor pronÛstico independiente. Braun et al. (26) han seÒalado que la detecciÛn de micromet·stasis en mÈdula Ûsea tiene evidente correlaciÛn con la mala evoluciÛn clÌnica de las pacientes.
Por ˙ltimo, la aplicaciÛn de nuevos procedimientos tecnolÛgicos, que dan lugar a los mÈtodos conocidos como microarrays y proteomics, podr·n aportar, en un futuro a mediano plazo, elementos pronÛsticos nuevos y m·s precisos de seleccionar el tratamiento adyuvante.
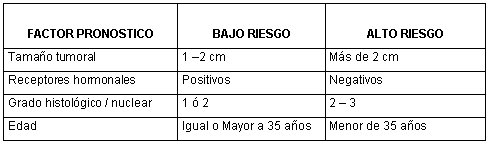
Las categorÌas de riesgo constituyen una manera ˙til de establecer en cada paciente el tratamiento adyuvante m·s adecuado. Estas categorÌas se correlacionan con la sobrevida que cada grupo alcanza al cabo de 5 y 10 aÒos de seguimiento, luego de tratamiento locorregional, asÌ como con las mejorÌas obtenidas con el tratamiento adyuvante sistÈmico. En la SÈptima Conferencia Internacional sobre Tratamiento Adyuvante del C·ncer de Mama, St. Gallen 2001 (3), se establecieron dos categorÌas: bajo riesgo y alto riesgo. La presencia de met·stasis ganglionares define el alto riesgo de las pacientes. Para las portadoras de c·ncer de mama sin met·stasis ganglionares, las caracterÌsticas del tumor o de la paciente que se seÒalan permiten definir los subgrupos de bajo y alto riesgo (Tabla No. 1).
Tabla 1. C·ncer de Mama sin Met·stasis Ganglionares. Grupos de Riesgo.
El NIH/NCI realizÛ la Conferencia de Consenso en el Tratamiento Adyuvante para el C·ncer de Mama en noviembre de 2000 (27). En ella se estableciÛ que los factores pronÛsticos de valor crÌtico para determinar el riesgo de recurrencia son: edad; estado de los ganglios axilares; tamaÒo tumoral; tipo histolÛgico / grado nuclear; receptores hormonales.
El objetivo del tratamiento hormonal adyuvante es el de impedir que las cÈlulas del carcinoma de mama reciban el estÌmulo estrogÈnico. Esta situaciÛn ocurre en los tumores que presentan receptores hormonales positivos. El reducido subgrupo de pacientes que no tienen receptores de estrÛgenos, pero contienen el receptor de progesterona, tambiÈn se beneficia del tratamiento hormonal adyuvante.
La deprivaciÛn estrogÈnica se puede obtener:
M˙ltiples ensayos clÌnicos han demostrado el beneficio del uso de tamoxifeno en las pacientes con c·ncer de mama que expresen receptores hormonales positivos, en forma independiente de la edad, estado menop·usico, presencia o ausencia de met·stasis ganglionares, tamaÒo del tumor y tratamiento con quimioterapia.
Las ˙nicas excepciones que se seÒalan son: tumores muy pequeÒos, de 1 cm de di·metro o menos; premenop·usicas que quieran evitar los sÌntomas de la deprivaciÛn estrogÈnica; postmenop·usicas que tengan historia clÌnica de episodios de trombosis venosas y de tromboembolismo pulmonar.
El beneficio observado significÛ una prolongaciÛn de la sobrevida global, asÌ como en la sobrevida libre de enfermedad con sustanciales reducciones en la posibilidad de recurrencia tumoral, de segundo c·ncer primitivo de mama y descenso de la mortalidad hasta los 15 aÒos de seguimiento. Estas conclusiones han sido seÒaladas por el EBCTCG (28,29,30) y recientemente, en la SÈptima ReuniÛn Internacional de St. Gallen (3).
En mujeres portadoras de c·ncer de mama con receptores hormonales positivos se observÛ que el tamoxifeno reduce la muerte por c·ncer de mama en 9% ± 1,5% a 15 aÒos, sin aumentar significativamente las muertes producidas por causas diferentes al c·ncer de mama.
SÛlo las pacientes con tumores con receptores hormonales positivos se beneficiaron del tratamiento con tamoxifeno. Por ello, se recomienda no utilizar tamoxifeno en las portadoras de tumores con receptores hormonales negativos (31). Esa recomendaciÛn se ve reforzada por los resultados del estudio del NSABP B-23 (32) y del Intergrupo (33), los que seÒalaron la no reducciÛn de la incidencia de c·ncer de mama contralateral o mejorÌa en la sobrevida global en pacientes con tumores receptores hormonales negativos.
El metaan·lisis del EBCTCG del aÒo 2000 estableciÛ la duraciÛn Ûptima del tratamiento adyuvante con tamoxifeno y demostrÛ que 5 aÒos de tratamiento (34,35,36), comparados con 1-2 aÒos, produjeron un incremento adicional en la sobrevida de 3,2% ± 1%, a los 10 aÒos, con sÛlo un aumento del 0,1% en los efectos colaterales graves, como el embolismo pulmonar y c·ncer de endometrio.
Por tanto se debe recomendar de rutina la duraciÛn de 5 aÒos de tratamiento. La prolongaciÛn del tratamiento con tamoxifeno adyuvante durante m·s de 5 aÒos no ha revelado a˙n un claro beneficio terapÈutico (37,38). Se contin˙a con la agrupaciÛn de pacientes en 2 ensayos clÌnicos importantes: aTTomb (39) y ATLAS (40). La dosis diaria cl·sicamente establecida es de 20 mg por dÌa y por vÌa oral.
El valor de la quimioterapia asociada al tamoxifeno se eval˙a en diversos estudios (41). En las pacientes postmenop·usicas, tanto los regÌmenes que contienen CMF en las dosis adecuadas (42) como los que contienen antraciclinas, tales como AC y FAC, mejoran la sobrevida libre de enfermedad (32,43), y probablemente la sobrevida global; se utilizan habitualmente en combinaciÛn con tamoxifeno en mujeres con receptores de estrÛgeno y de progesterona positivos.
Se ha demostrado que se debe administrar el tamoxifeno de manera secuencial y no concurrente con la quimioterapia (43,44,45), a continuaciÛn de esa adyuvancia.
Los inhibidores de la aromatasa de tercera generaciÛn, como anastrozole (Arimidex), letrozole (Femara) y exemestano (Aromasin), han demostrado su valor terapÈutico en el c·ncer de mama metast·sico, en mujeres post menop·usicas. Esos resultados han determinado un notorio interÈs por utilizarlos en el tratamiento adyuvante, lo que ha dado origen a ensayos aleatorios, como ATAC, en el que se compara anastrazol (A) con tamoxifeno (T) y con la combinaciÛn de ambos (AT), en pacientes postmenop·usicas con receptores positivos o desconocidos. Se ha completado el grupo de pacientes, pero hay que aguardar los resultados con un seguimiento prolongado. Otros ensayos en curso comparan exemestano versus tamoxifeno, letrozole versus placebo despuÈs de 5 aÒos de tamoxifeno adyuvante en pacientes postmenop·usicas, o tamoxifeno versus exemestano como primera opciÛn en hormonoterapia adyuvante, o faslodex versus tamoxifeno.
La ablaciÛn ov·rica es un tratamiento hormonal de alternativa para las pacientes premenop·usicas (46,47). En el metaan·lisis del EBCTCG de 2000, (9,48,49), se seÒala que la ablaciÛn ov·rica efectuada por diferentes procedimientos (cirugÌa, radioterapia o farmacolÛgica) prolonga la sobrevida global absoluta, a 15 aÒos, en 10,4% +/- 3,1%, en pacientes menores de 50 aÒos, en las que se comparÛ la ablaciÛn ov·rica con un grupo control sin tratamiento. En los ensayos clÌnicos en los que se cotejÛ la ablaciÛn ov·rica con diversos regÌmenes de quimioterapia adyuvante convencional: CMF (50,51,52,53); FAC (54); FEC (55), no se evidenciaron diferencias en la sobrevida.
La asociaciÛn de quimioterapia y ablaciÛn ov·rica versus quimioterapia no ha establecido a˙n una ventaja en la sobrevida a favor del tratamiento combinado (56). Por el momento, se debe considerar que la ablaciÛn ov·rica es un tratamiento adyuvante aceptable en mujeres premenop·usicas con c·ncer de mama hormonorrespondedor. Hacen falta nuevos estudios prospectivos que establezcan si la ablaciÛn ov·rica es aditiva cuando se la combina con tamoxifeno o con quimioterapia.
El desarrollo de los an·logos LHRH ha despertado creciente interÈs. La goserelina (Zoladex) en c·ncer de mama metast·sico mostrÛ eficacia terapÈutica comparable a la castraciÛn quir˙rgica (57). La asociaciÛn con tamoxifeno m·s un an·logo LHRH fue superior al an·logo LHRH empleado solo (58). Esos resultados han motivado su uso como tratamiento adyuvante (59). El m·s empleado fue la goserelina (Zoladex). Se la ha comparado con tamoxifeno o goserelina m·s tamoxifeno o quimioterapia, o a Èsta m·s tamoxifeno o m·s goserelina versus goserelina m·s tamoxifeno m·s quimioterapia (60).
El ensayo ZIPP (61), en premenop·usicas, observÛ, con 4,3 aÒos de seguimiento, 20% menos de recurrencia en las pacientes que recibieron goserelina, independiente del uso concurrente de tamoxifeno o quimioterapia.
El estudio ECOG (56), en que se comparÛ CAF con CAF/goserelina con CAF/goserelina/tamoxifeno en premenop·usicas con ganglios positivos, demostrÛ que la triple combinaciÛn fue superior en sobrevida libre de enfermedad, pero sin diferencia en la sobrevida global.
El Zoladex Early Breast Cancer Research Association (ZEBRA) (62), en premenop·usicas con ganglios positivos, comparÛ CMF con 2 aÒos de goserelina. En este estudio, luego de 6 aÒos de seguimiento, en el grupo de pacientes con receptores de estrÛgeno positivos, la goserelina fue equivalente a CMF en sobrevida libre de enfermedad; en cambio, en el subgrupo de receptores negativos, CMF fue superior a goserelina. La sobrevida global fue similar en ambos grupos.
Del conjunto de los resultados conocidos se puede estimar que la goserelina se asocia con una reducciÛn significativa en las recurrencias; en mortalidad, el efecto es sÛlo marginal.
La quimioterapia es el tratamiento adyuvante de elecciÛn para la mayorÌa de las pacientes con receptores hormonales negativos. En el metaan·lisis del EBCTCG de 1998 (63) y en su actualizaciÛn de 2000 (48), todos los subgrupos de pacientes, ganglios negativos o ganglios positivos, pre o postmenop·usicas, con receptores hormonales negativos o positivos, se benefician significativamente en la sobrevida global, con rangos de 3% a 12%. El beneficio es mayor en las mujeres con mayor riesgo de recidiva.
Los datos del Surveillance Epidemiology and End Results (SEER) (64) seÒalan que aquellos tumores menores de 1 cm de di·metro y con ganglios negativos presentan una sobrevida a 8 aÒos de 95%, con pronÛstico excelente e independiente del grado tumoral, por lo que no necesitarÌan quimioterapia adyuvante. Por el contrario, una revisiÛn de protocolos del NSABP en pacientes con ganglios negativos, aleatorios, frente a un grupo control con quimioterapia adyuvante, demostrÛ que los tumores de 1 cm de di·metro o menos, con receptores hormonales negativos, tenÌan peor pronÛstico cuando no recibÌan quimioterapia adyuvante (sobrevida libre de enfermedad a 8 aÒos: 90% versus 81%; p=0,06) (65).
En funciÛn de estos datos, la Conferencia de Consenso del NHI/NCI (27) , estima que esa terapia adyuvante tal vez no sea necesaria en tumores menores de 1 cm con ganglios negativos, con histologÌa favorable (tipo tubular o mucinoso) y en pacientes mayores de 70 aÒos.
En los restantes grupos de tumores, con di·metro mayor de 1 cm (27) o mayor de 2 cm (2,3), la reducciÛn de la recidiva se comprueba en los 5 primeros aÒos y persiste luego de ese lapso, pero sin incrementarse. La mejorÌa en la sobrevida global se constata en los 5 primeros aÒos, pero con un beneficio adicional en los 6 aÒos subsiguientes. Las reducciones significativas de las recurrencias y de la mortalidad se comprueban en pacientes tanto jÛvenes como mayores, aunque la reducciÛn es proporcionalmente menor en las pacientes de m·s edad.
En las menores de 50 aÒos, el beneficio que se obtiene con la quimioterapia adyuvante es similar en quienes presentan receptores hormonales positivos o negativos. En el grupo etario de 50 a 69 aÒos, se comprobÛ una significativa reducciÛn en las recurrencias y en la mortalidad con quimioterapia adyuvante, tanto en portadoras de tumores receptores hormonales positivos como negativos (43,69,70,71,72). En ellas, el descenso en las recurrencias fue el doble en receptores hormonales negativos y la diferencia frente a las pacientes con receptores hormonales positivos fue significativa.
Con relaciÛn a las pacientes que presentaron met·stasis en los ganglios, la reducciÛn proporcional en recurrencias y mortalidad fue similar en las pacientes con receptores hormonales positivos y con receptores negativos. En pacientes menores de 50 aÒos, el beneficio terapÈutico fue mayor en quienes presentaron met·stasis ganglionares (11%) contra 7% en quienes no las presentaron. En las mujeres de 50 a 69 aÒos de edad, el beneficio alcanzado en la reducciÛn de las recurrencias a 10 aÒos fue parecido: 2% en ganglios negativos y 3% en ganglios positivos. En este mismo subgrupo, en cambio, la reducciÛn de la mortalidad fue mayor en las pacientes con met·stasis ganglionares.
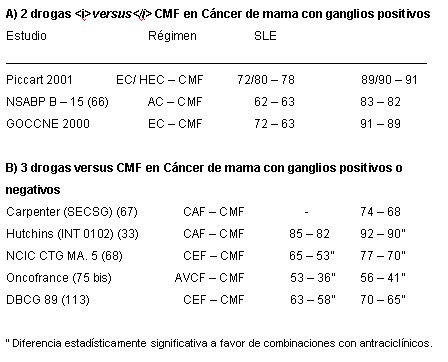
La comparaciÛn entre los regÌmenes de quimioterapia que contienen antraciclÌnicos y los de tipo CMF mostrÛ una reducciÛn proporcional de las recurrencias, de 12% y de 11% en la mortalidad a favor del uso de las antraciclinas (63). El riesgo absoluto de recidiva se redujo en 3,2% y el de mortalidad, en 2,7%. Al respecto, el estudio comparativo de la eficacia de combinaciones de antraciclÌnicos versus CMF en portadoras de c·ncer de mama con met·stasis ganglionares (3,32,33,66,68,69,75,76,77) da resultados equivalentes en regÌmenes antraciclÌnicos de 2 drogas, pero mejores en regÌmenes triples (Tabla No. 2).
Tabla 2. Analisis Comparativo de RegÌmenes con Antraciclinicos versus Cmf.
La importancia terapÈutica de las dosis Ûptimas de la quimioterapia adyuvante, con miras a lograr el mejor beneficio terapÈutico, se ha reiterado recientemente en Lohrisch et al. (78) y Basser (79).
En la conferencia de consenso de NHI/NCI (1) se ratifica una serie de aspectos Ìntimamente relacionados con la elecciÛn de la quimioterapia adyuvante, tales como la recomendaciÛn de elegir un rÈgimen con dos o m·s drogas y no esquemas de monodroga. La duraciÛn que se propone es 4 a 6 ciclos de quimioterapia durante 3 a 6 meses (80). Los esquemas que se recomiendan son AC, CEF/ FEC, CAF/ FAC, A ñ CMF. Se debe considerar siempre el uso de tamoxifeno adyuvante en las pacientes con tumores con receptores hormonales positivos que tengan indicaciÛn de quimioterapia adyuvante.
En cuanto al concepto de intensidad de dosis o cantidad de droga suministrada por unidad de tiempo, est· correlacionado con la respuesta al tratamiento (81). En el estudio CALGB 8541 se evaluÛ tres niveles de dosis y se demostrÛ efectos significativos en tÈrminos de sobreviva sÛlo con los niveles intermedios y altos (82). Bonneterre et al. (83) evaluaron la eficacia de FEC con epirrubicina 50 mg/m2 versus 100 mg/m2, y se comprobÛ un efecto claramente significativo con la dosis mayor. El an·lisis minucioso de esta informaciÛn permite afirmar que hay niveles crÌticos de dosificaciÛn de los citost·ticos por debajo de los cuales Èstos serÌan ineficaces.
El estudio CALGB 9344, en mujeres con met·stasis ganglionares, asignÛ aleatoriamente a tres niveles diferentes de doxorrubicina: 60, 75 y 90 mg/m2 (84), y demostrÛ ausencia de beneficio terapÈutico con el aumento de dosis por sobre 60 mg/m2 de doxorrubicina. El estudio NSABP B-22 tampoco logrÛ demostrar mayor acuvidad con el escalamiento de las dosis de ciclofosfamida (85). El estudio NSABP B-25 explorÛ el incremento en la intensidad de dosis y en la dosis acumulativa de ciclofosfamida, sin obtener beneficio terapÈutico (86).
El concepto de densidad de dosis tambiÈn se ha ensayado (87). Bonadonna et al. (88), en pacientes con m·s de tres ganglios con met·stasis, compararon A y CMF en esquema alternante o secuencial. Al dÈcimo aÒo, esta ˙ltima combinaciÛn, que era m·s intensa en cuanto a densidad de dosis, demostrÛ que era superior.
La sobreexpresiÛn de Her-2 neu (c-erb B-2) est· seÒalada en estudios retrospectivos como predictor de respuesta a la quimioterapia con antraciclÌnicos (89), aunque estudios posteriores (90) no lograron confirmar esa correlaciÛn. Otros estudios clÌnicos aportan resultados parciales beneficiosos en relaciÛn al uso de antraciclÌnicos, en tumores con estas caracterÌsticas, tales como el NSABP B ñ 11 (91), el CALGB 8082 (92) y el NSABP B ñ 15 (93). Si bien todos los estudios mencionados no tienen resultados con significaciÛn estadÌstica, los autores estiman que hay una clara tendencia en el beneficio terapÈutico que aporta la doxorrubicina en las pacientes con tumores HER 2 positivos.
Como contrapartida, la interacciÛn entre la sobreexpresiÛn de HER 2 y la quimioterapia con CMF demostrÛ que el beneficio terapÈutico se comprobÛ en pacientes HER 2 negativas (94,95).
El valor terapÈutico del trastuzumab (Herceptin) en c·ncer de mama metast·sico HER 2 positivo ha sido la base de su incorporaciÛn en ensayos prospectivos para el tratamiento adyuvante en los tumores que sobreexpresan el gen, tales como son NSABP B-31 (96), BCIRG 006 (97), HERA (98), NCIC-CTG y E 2198, actualmente en marcha. Mientras no se disponga de sus resultados, el trastuzumab se deber· emplear en el contexto de estudios clÌnicos de investigaciÛn (99).
Si bien los taxanos son agentes tan activos como la doxorrubicina, en el tratamiento de la enfermedad metast·sica, su papel en el tratamiento adyuvante no est· definitivamente establecido (100). El ensayo clÌnico CALGB 9344 (84), comunicado en el Consenso NIH/NCI (101), comprobÛ que, a 52 meses de seguimiento, la mejorÌa en la sobreviva global informada anteriormente en las pacientes tratadas con AC/Paclitaxel versus AC, sÛlo tenÌa significaciÛn estadÌstica en el lÌmite de su valor (1,27,102). En el estudio NSABP B ñ 28 (103), que compara AC/Paclitaxel con AC, no se demostraron diferencias a 34 meses de seguimiento. El estudio del M D Anderson, (104) que compara FAC con Paclitaxel/FAC, tampoco comprobÛ diferencias a 36 meses de seguimiento. Hay a la fecha otros 12 estudios cooperativos en marcha, por lo que la incorporaciÛn de los taxanos a la quimioterapia adyuvante no se puede considerar a˙n una terapÈutica est·ndar (106).
En pacientes con numerosos linfonodos axilares positivos, en las cuales hay un mal pronÛstico con la quimioterapia adyuvante tradicional, algunos autores plantean el uso de esquemas que incluyan taxanos.
La quimioterapia de altas dosis, con rescate con cÈlulas progenitoras, se encuentra tambiÈn en fase de evaluaciÛn. La ˙ltima comunicaciÛn de Peters no logrÛ demostrar beneficio con su utilizaciÛn (107); lo mismo ocurriÛ con una serie de otras publicaciones, incluso el estudio escandinavo SBG 9401 (100), el Dutch Nacional Study (109,110), el del Netherlands Cancer Institute (109,110) y el de M D Anderson (112), por lo que se debe estimar que es una tecnologÌa absolutamente experimental.
Por ˙ltimo, debemos considerar en el desarrollo futuro de la quimioterapia adyuvante la incorporaciÛn de otros agentes citost·ticos de alta efectividad en el terreno de la enfermedad metast·sica, como la vinorelbina y otras, que permitir·n ampliar las espectativas terapÈuticas actuales en el manejo de esta enfermedad.
Los datos aportados por las sucesivas revisiones del EBCTCG (9,28,29,30,46,47,48,49,63), asÌ como las recomendaciones terapÈuticas propuestas en St. Gallen (2,3) y por la Conferencia de Consenso del NIH/NCI (1,27,102), permiten delinear las recomendaciones para los estadios I y II, incluyendo algunos casos del estadio III A:
1.- C·ncer de Mama con Met·stasis Ganglionares
Para las pacientes receptores hormonales positivos, menores de 35 aÒos, se recomienda el uso de tamoxifeno, adem·s de la quimioterapia, dados los resultados poco satisfactorios obtenidos con el empleo ˙nico de quimioterapia.
El esquema CMF se puede utilizar cuando haya contraindicaciÛn para el uso de antraciclÌnicos. El empleo del esquema AC por 4 ciclos no es el tratamiento apropiado para el grupo con ganglios metast·sicos. Las recomendaciones se centran en esquemas que incluyan antraciclÌnicos: FAC o CAF; FEC; A-CMF secuencial; AC-Paclitaxel secuencial. El n˙mero de ciclos variar· entre 6 y 8, seg˙n la combinaciÛn elegida.
2. C·ncer de Mama sin Met·stasis Ganglionares
Se debe definir, en primer lugar, las categorÌas de riesgo, de acuerdo a las recomendaciones m·s recientes (1,3):
Las recomendaciones terapÈuticas para este grupo son:
Pacientes de bajo riesgo. Tumores con receptores hormonales positivos, pre o post menop·usicas: Tamoxifeno o nada.
Para las pacientes portadoras de tumores pequeÒos sin met·stasis ganglionares y con histologÌa favorable, tubular o mucinoso, no se recomienda adyuvancia.
Pacientes de alto riesgo.
Tumores con Receptores Hormonales Positivos
Premenop·usicas:
Postmenop·usicas:
Tumores con Receptores Hormonales Negativos pre o postmenop·usicas: quimioterapia
Los regÌmenes que contienen antraciclÌnicos son los de elecciÛn para el tratamiento adyuvante en pacientes de alto riesgo con ganglios negativos. Se debe tener presente que 4 ciclos de AC equivalen a 6 ciclos de CMF, como quimioterapia adyuvante en pacientes de alto riesgo sin met·stasis ganglionares (32).
 Esta obra de Medwave est· bajo una licencia Creative Commons AtribuciÛn-NoComercial 3.0 Unported. Esta licencia permite el uso, distribuciÛn y reproducciÛn del artÌculo en cualquier medio, siempre y cuando se otorgue el crÈdito correspondiente al autor del artÌculo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave est· bajo una licencia Creative Commons AtribuciÛn-NoComercial 3.0 Unported. Esta licencia permite el uso, distribuciÛn y reproducciÛn del artÌculo en cualquier medio, siempre y cuando se otorgue el crÈdito correspondiente al autor del artÌculo y al medio en que se publica, en este caso, Medwave.
Este texto completo es la transcripciÛn editada y revisada de una conferencia dictada en las Jornadas Latinoamericanas de C·ncer de Mama 2002, organizadas por la Escuela Latinoamericana de MastologÌa, FederaciÛn Latinoamericana de MastologÌa y Sociedad Chilena de MastologÌa.
Editor CientÌfico: Dr. Hernando Paredes.
Expositor:
Carlos Garbino[1]
CitaciÛn: Garbino C. Systemic adjuvant treatment of breast cancer: stages I and II. Medwave 2003 Sep;3(8):e3333 doi: 10.5867/medwave.2003.08.3333
Fecha de publicaciÛn: 1/9/2003
Nos complace que usted tenga interÈs en comentar uno de nuestros artÌculos. Su comentario ser· publicado inmediatamente. No obstante, Medwave se reserva el derecho a eliminarlo posteriormente si la direcciÛn editorial considera que su comentario es: ofensivo en alg˙n sentido, irrelevante, trivial, contiene errores de lenguaje, contiene arengas polÌticas, obedece a fines comerciales, contiene datos de alguna persona en particular, o sugiere cambios en el manejo de pacientes que no hayan sido publicados previamente en alguna revista con revisiÛn por pares.
A˙n no hay comentarios en este artÌculo.
Para comentar debe iniciar sesiÛn
Medwave publica las vistas HTML y descargas PDF por artÌculo, junto con otras mÈtricas de redes sociales.
Eifel P, Axelson JA, Costa J, Crowley J, Curran WJ Jr, Deshler A, et al. National Institutes of Health consensus Development Panel. National Institutes of Health Consensus Development Conference Statement: Adjuvant Therapy for Breast Cancer, November 1-3, 2000. J Natl Cancer Inst. 2001 Jul 4;93(13):979-89. | CrossRef | PubMed |Goldhirsch A, Glick JH, Gelber RD, Senn HJ. Goldhiresh A, Glick JH, Gelber RD, Senn HJ : ìMeeting highlights: International Consensus Panel on the Treatment of Primary Breast Cancer. J Natl Cancer Inst. 1998 Nov 4;90(21):1601-8. | CrossRef | PubMed |St. Gallen 2001 News. Ed. Phillips Group Oncology Communications Co. PO Box 4024. Philadelphia, PA. USA, Decatron Digital Vision, Decatron Media AG | Link |Fitzgibbons PL, Page DL, Weaver D, Thor AD, Allred DC, Clark GM, et al. Prognostic Factors in Breast Cancer: College of American Pathologists Consensus Statement 1999. Arch Pathol Lab Med. 2000 Jul;124(7):966-78. | PubMed |Clark GM. Prognostic and predictive factors. En: Diseases of the breast. Philadelphia. PA. Lippincott Williams and Wilkins, 2000, 489ñ514. Reed W, Hannisdal E, Boehler PJ, Gundersen S, Host H, Marthin J. The prognostic value of p53 and c ñ erb ñ B2 immunostaining is overrated for patients with lymph node negative breast carcinoma: a multivariate analysis of prognostic factors in 613 patients with a follow -up of 14 ñ 30 years. Cancer. 2000 Feb 15;88(4):804-13. | CrossRef | PubMed |Volpi A, De Paola F, Nanni O, Granato AM, Bajorko P, Becciolini A, et al. Prognostic significance of biologic marñKers in nodeñnegative breast cancer patients: a prospective study. Breast Cancer Res Treat. 2000 Oct;63(3):181-92. | CrossRef | PubMed |Rudolph P, Olsson H, Bonatz G, Ratjen V, Bolte H, Baldetorp B, et al. Correlation between p53, cñerbñB2 and topoisomerasa II alpha expression, DNA ploidy, hormonal receptor status and proliferation in 356 nodeñnegative breast carcinomas: prognostic implications. J Pathol. 1999 Jan;187(2):207-16. | CrossRef | PubMed |Kroman N, Jensen MB, Wohlfahrt J, Mouridsen HT, Andersen PK, Melbye M. Factors influencing the effect of age on prognosis in breast cancer: Population based study. BMJ. 2000 Feb 19;320(7233):474-8. | CrossRef | PubMed | PMC |Ferrero JM, Ramaioli A, Formento JL, Francoual M, Etienne MC, Peyrottes I, et al. P53 determination alongside classical prognostic factors in nodeñnegative breast cancer: an evaluation at more than 10 year follow-up. Ann Oncol. 2000 Apr;11(4):393-7. | CrossRef | PubMed |Hamilton A, Piccart M. The contribution of molecular markers to the prediction of response in the treatment of breast cancer: a review of the literature on Herñ2, p 53 and BCLñ2. Ann Oncol. 2000 Jun;11(6):647-63. | CrossRef | PubMed |Amadori D, Nanni O, Marangolo M, Pacini P, Ravaioli A, Rossi A, et al. Diseaseñfree survival advantage of adjuvant cyclophosphamide, methotrexate and fluorouracil in patients with nodeñnegative, rapidly proliferating breast cancer: a randomized multicenter study. J Clin Oncol. 2000 Sep;18(17):3125-34. | PubMed |Jones S, Clark G, Koleszar S, Ethington G, Mennel R, Paulson S, et al. Low proliferative rate of invasive node- negative breast cancer predicts for a favourable outcome without adjuvant chemotherapy. Clin Breast Cancer. 2001 Jan;1(4):310-4; discussion 315-7.
http://dx.doi.org/10.3816/CBC.2001.n.005 | PubMed |Trock BJ, Yamauchi H, Brotzman M et al. cñerbñB2 as a prognostic factor in breast cancer (BC): a meta-analysis. Proc Am Soc Clin Oncol. 2000; 19:7 Hayes DF, Yamauchi H, Stearns V et al.Should all breast cancers be tested for cñerbñB2? En: American Society of Clinical Oncology Educational Book. 36 th Annual Meeting. Alexandria, VA. USA. American Society of Clinical Oncology 2000, 257ñ265. StÂl O, Borg A, Fernˆ M, K‰llstrˆm AC, Malmstrˆm P, Nordenskjˆld B, et al. Erb B2 status and benefit from two or five years of adjuvant tamoxifen in post-menopausal early breast cancer. Ann Oncol. 2000 Dec;11(12):1545-50. | CrossRef | PubMed |Paik S, Bryant J, Tan-Chiu E, Yothers G, Park C, Wickerham DL, et al. Her 2 and choice of adjuvant chemotherapy for invasive breast cancer: National Surgical Adjuvant Breast and Bowel Project protocol B-15. J Natl Cancer Inst. 2000 Dec 20;92(24):1991-8. | CrossRef | PubMed |Andrulis IL, Bull SB, Blackstein ME, Sutherland D, Mak C, Sidlofsky S, et al. neu/erb Bñ2 amplification identifies a poorñprognosis group of women with node negative breast cancer. J Clin Oncol. 1998 Apr;16(4):1340-9. | PubMed |Rosen PP, Groshen S, Kinne DW, Norton L. Factors influencing prognosis in node-negative breast carcinoma; analysis of 767 T1N0M0/ T2N0M0 patients with long-term follow-up. J Clin Oncol. 1993 Nov;11(11):2090-100. | PubMed |Eppenberger U, Kueng W, Schlaeppi JM, Roesel JL, Benz C, Mueller H, et al. Markers of tumor angiogenesis and proteolysis independently define high- and low-risk subsets of node-negative breast cancer. J Clin Oncol. 1998 Sep;16(9):3129-36. | PubMed |Foekens JA, Peters HA, Look MP, Portengen H, Schmitt M, Kramer MD, et al. The urokinase system of plasminogen activation and prognosis in 2780 breast cancer patients. Cancer Res. 2000 Feb 1;60(3):636-43. | PubMed |Harbeck N, Thomssen C, Berger U, Ulm K, Kates RE, Hˆfler H, et al. Invasion marker PAIñ1 remains a strong prognostic factor after long-term follow-up both for primary breast cancer and following first relapse. Breast Cancer Res Treat. 1999 Mar;54(2):147-57.
| CrossRef | PubMed |Prechtl A, Harbeck N, Thomssen C, Meisner C, Braun M, Untch M, et al. Tumor-biological factors uPA and PAIñ1 as stratification criteria of a multicenter adjuvant chemotherapy trial in node-negative breast cancer. Int J Biol Markers. 2000 Jan-Mar;15(1):73-8. | PubMed |Thomssen C, Prechtl A, Meisner C, et al. Efficacy of adjuvant chemotherapy in node-negative breast cancer patients with elevated uPA and PAIñ1. tumor S67, Abstract 133. Braun S, Pantel K, M¸ller P, Janni W, Hepp F, Kentenich CR, et al. Cytokeratin-positive cells in the bone marrow and survival of patients with stage I, II or III breast cancer. N Engl J Med. 2000 Feb 24;342(8):525-33. | CrossRef | PubMed |Abrams JS. Overview of the US consensus conference on adjuvant therapy for breast cancer. The Breast 2001; 10 (supplement 3): 139 ñ 146. Effects of adjuvant tamoxifen and cytotoxic therapy on mortalitv early breast cancer: an overview of 61 randomized trials among 28.896 women. N Engl J Med. 1988 Dec 29;319(26):1681-92. | CrossRef | PubMed |Systemic treatment of early breast cancer by hormonal, cytotoxic or immune therapy: 133 randomized trials involving 31.000 recurrences and 24.000 deaths among 75.000 women. Lancet. 1992 Jan 11;339(8785):71-85. | PubMed |Tamoxifen for early breast cancer: an overview of the randomized trials. Lancet. 1998 May 16;351(9114):1451-67. | CrossRef | PubMed |Fisher B, Digman J, Wiensd S, Wolmark N, wickerham DL. Duration of tamoxifent (TAM) therapy for primary breast cancer: 5 years versus 10 years (NSAPP) P-14. Proc Am Soc Clin Oncol. 1996; 15:113 (Abstract). Fischer B., Anderson s, Wolmark N, Tan-Chiu E. Chemoterapy with or without tamoxifen for patients with ER-negative breast cancer and negative nodes: Results from NSABP B-23. Proc Am Soc Clin Oncol. 2000; 19:72. (Abstract). Hutchins L, Green S, Ravdin P. CMF versus CAF with and without tamoxifen in high-risk node-negative breast cancer patients and a natural history fallow-up study in low-risk node-negative patients: first results of intergroup trial INT 0102. Proc Am Soc Clin Oncol 1998; 17:1. (Abstract). Delozier T, Spielmann M, Mace-Lesech J et al.Short-term versus lifelong adjuvant tamoxifen in early breast cancer (EBC): A randomized trial (TAM-01). Proc Am Soc Clin Oncol 1997; 16: 1289. Gallen M, Alonso MC, Ojeda B et al. ìRandomized multicentre trial comparing two different time-spans of adjuvant tamoxifen therapy (ATT) in women with operable node positive breast cancerî, Proc Am Soc Clin Oncol 1994; 13: 76(abst). Randomized trial of twa versus five years of adjuvant tamoxifen for postmenopausal early sta~e breast oancer. J Natl Cancer Inst. 1996 Nov 6;88(21):1543-9. | CrossRef | PubMed |Stewart HJ, Forrest AP, Everington D, McDonald CC, Dewar JA, Hawkins RA, et al. Randomized comparison of 5 years of adjuvant tamoxifen with continuous therapy for operable breast. Br J Cancer. 1996 Jul;74(2):297-9. | CrossRef | PubMed |Tormey DC, Gray R, Falkson HC. Postchemotherapy adjuvant tamoxifen beyond five years in patients with lymph node-positive breast cancer. J Natl Cancer Inst. 1996 Dec 18;88(24):1828-33. | CrossRef | PubMed |CRC Trials Unit Birmingham. Adjuvant tamoxifen treatment offer more?(aTTom) Protocol. Birmingham: CRC Trials Unit.Clinical Research Block. Queen Elizabeth Hospital. Clinical Trial Service Unit, Radcliffe Infirmary, 0xford. Adjuvant tamoxifen longer against shorter (ATLAS). Protocol. April 1995. ATLAS Office,Clinical Trial Service Unit, Radcliffe lnfirmary,Oxford.(UK) Pritchard KI. Optimal endocrine therapy. The Breast 2001;10(Suppl 3):114ó122 Goldhirsch A, Coates AS, Colleoni M, Castiglione-Gertsoh M,Gelber RD. Adjuvant Chemoendocrine therapy in postmenopausal breast cancer:cyclophosphamide, metothrexate and fluorouracil dose and schedule may make a difference. J Clin Oncol. 1998 Apr;16(4):1358-62. | PubMed |Albain K,Green S,Osborne K. et al.Tamoxifen (T) versus cyclophosphamide adriamycin and 5-Fu plus either concurrent or sequential T in postmenopausal receptor (positive) or node (positive) breast cancer: A Southwest Onoology Group phase III intergroup trial (SWOG-8814,INT-0100) Proc Am Soc Clin Oncol l997;16:128a. (Abstract). Osborne CK :Effects of estrogen and antiestrogens on cell proliferation. Implications for treatment of breast cancer. Endocrine treatment in breast and prostate cancer. OWSBORNE ck, ED. Kluwer, Boston, Massachussets, USA 1988: 11-129. Ovarian ablation in early breast cancer: An overview of randomized. Trials. Lancet. 1996 Nov 2;348(9036):1189-96. | CrossRef |Ovarian ablation for early breast cancer (Cochrane review). Cochrane Database Syst Rey 2000; 3:CD 000485. Early Breast Cancer Trialistsí Collaborative Group (EPCTCG) 2000 analysis overvlew results. Fifth Meeting of the Early Breast Canoer Trialistsí Collaborative Group. 2000 Oxford Peto R: Early Breast Cancer Trialistsí Collaborative Group Meeting. Oxford, October 2000. Adjuvant ovarian ablation CMF chemotherapy in premenopausal women with pathological stage II breast carcinoma: the Scottish trial. Lancet. 1993 May 22;341(8856):1293-8. | PubMed |Ejlertsen B,Dombernowsky P, Mouridsen H. et al. Comparable effect of ovarian (OA) and CNF chemotherapy in premenopausal hormonal receptor positive breast cancer patients (prp) Proc Am Sao Clin Oncol l999; 18: 66a (Abstract) Jonat W. Zoladex (Goserelin) vs CMF as adjuvant therapy in pre/perimenopausal early node-positive breast oancer:preliminary efficacy, COL,and PMD results from the ZEBRA Study. Breast Can Res Treat 2000;1:20 (Abstract) Jakesz R, Gnant M,Hausmaninger H et al. Combination goserelin and tamoxifen is more effective than CMF in premenopausal patients with hormone-responsive tumors in a multicentre trial of the Austrian Breast Cancer Study Group (APCSG) Breast Cancer Res Treat 1999; 57:25. Roche H,Mihura J,de Cafontan B et al. Castration and tamoxifen versus chemotherapy. (FAC) for premenopausal, node and receptor-positive breast cancer patients: a randomized trial with a 7 years median follow-up. Proc Am Soc Clin Oncol 1996;15:117 (Abstract) Roche H,Keibrat P, Bonneterre J et al. Complete hormonal blockade versus chemotherapy in premenopausal early stage breast cancer patients (Pts) with positive hormone-reoeptors (HR+, ) and 1-3 node-positive (N+) tumor, results of the FASG 06 trial. Proc Am Soc Clin Oncol 2000;19:72a (Abstract). Davidson N,OíNeill A,Vukov A et al.Effect of chemo-hormonal therapy in premenopausal node (positive) receptor (positive) breast cancer: an Eastern Cooperative 0ncology Group Phase III Intergroup Trial (E 5128,INT-0101)Proc Am Soc Clin Oncol 1999; l8:67a (Abstract). Taylor CW, Green S, Dalton WS, Martino S, Rector D, Ingle JN, et al. Multicentre randomized clinical trial of goserelin versus surgical ovariectomy in premenopausal patients with receptor-positive metastatic breast cancer: An Intergroup study. J Clin Oncol. 1998 Mar;16(3):994-9. | PubMed |Boccardo F,Blamey R,Klijn J,Tominaga T,Duchateau L,Sylvester R. HRH-Agonist (LHRH-A) plus tamoxifen (TAM) versus LHRH-A alone in premenopausal women with advanced breast cancer (ABC) :Results of a meta-analysis of four trials#. Proc Am Soc Clin Oncol 1999;18:110a (Abstract). Kaufmann M,von Minckwitz G, for the German Adjuvant Breast Cancer Study Group (GABG). The emerging role of hormonal ablation as adjuvant therapy in node positive and node negative pre/perimenopausal patients. The Breast 2001; 10 (Suppl 3): 123-129. Randomized controlled trial of ovarian function supression plus tamoxifen versus the same endocrine the rapy plus chemotherapy: is chemotherapy necessary for premenopausal women with node-positive, endocrine-responsive breast cancer? First results of International Breast Cancer Study Group Trial 11-93. The Breast 2001;10 (Suppl 3): 130-138. Rutqvist LE. Zoladex and tamoxifen as adjuvant therapy in premenopausal breast cancer: A raridomized trial by the Cancer Research Campaign (CRC) Breast Cancer Trials Group, the Stockholm Breast Cancer Study Group, the South-East Sweden Breast Group and the Gruppo Interdisciplinaire Valutazione Interventi in 0ncologia (GIVIO). Proc Am Soc Clin Oncol 1999;18:67a (Abstract) Zoladex (Goserelin) Vs CMF as adjuvant therapy in pre/perimenopausa1, node-positive,early breast cancer: Preliminary efficacy results from the ZEBRA study. Breast 2001;10:S30. Polychemotherapy for early breast cancer: an overview of the randomized trials. Lancet. 1998 Sep 19;352(9132):930-42. | CrossRef | PubMed |Carter CL, Allen C,Henson DE. Relation of tumour size, lymph node status and survival in 24,750 breast cancer cases. Cancer. 1989 Jan 1;63(1):181-7. | CrossRef | PubMed |Fisher B, Dignam J, Tan-Chiu E, Anderson S, Fisher ER, Wittliff JL, et al. Prognosis and treatment of patients with breast turnors of one centimeter or less and negative axillary nodes. J Natl Cancer Inst. 2001 Jan 17;93(2):112-20. | CrossRef | PubMed |Fisher B, Brown AM, Dimitrov NV et al. Two months of doxorrubicin-cyclo phosphamide with and without interval reinduction therapy compared with 6 months of cyclophosphamide, methotrexate and fluorouracil in node-positive breast cancer patients with tamoxifen-nonresponsive tumors: results from :the National Surgical Adjuvant Breast and Bowel Project B-15 J Clin Oncol 1990 8:1483ó1496. | PubMed |Carpenter JT, Velwz-Garcia E, Aron BS et al. Five years results of a randomized comparison of cyclophospharnide, doxorrubicin and fluorouracil for node-positive breast cancer. Proc Am Soc Clin Oncol 1994;13:68 (Abstraet 20s). Levine MN, Bramwell VH, Pritchard KI, Norris BD, Shepherd LE, Abu-Zahra H, et al. Randomized trÌal of intensive cyclophosphamide, epirubicin and fluorouracil chemotherapy compared with cyclophosphamide, methotrexate and fluorouracil in premenopausal wotnen with node positive breast cancer. J Clin Oncol. 1998 Aug;16(8):2651-8. | PubMed |Fisher B, Redmond C, Legault-Poisson S, Dimitrov NV, Brown AM, Wickerham DL, et al. Postoperative chemotherapy and tamoxifen compared with tamoxifen alone in the treatment of positive-node breast cancer patients aged 50 years and. older with tumors responsive to tamoxifen: Results from the Nationa1 Surgical Adjuvant Breast and Bowel Project B-16. J Clin Oncol. 1990 Jun;8(6):1005-18. | PubMed |International Breast Cancer Study Group. Effectiveness of adjuvant chemotherapy in combination with tamoxifen for node-positive postmenopausal treast cancer patients. J Clin Oncol. 1997 Apr;15(4):1385-94 | PubMed |Crivellari D, Bonetti M, Castiglione-Gertsch M, Gelber RD, Rudenstam CM, Th¸rlimann B, et al. Burdens and benefits of adjuvant cyclophosphamide, methotrexate and fluorouracil and tamoxifen for elderly patients with breast cancer. The International Breast Cancer Study Group Trial VII. J Clin Oncol. 2000 Apr;18(7):1412-22. | PubMed |Fisher B, Dignam J, Wolmark N, DeCillis A, Emir B, Wickerham DL, et al. Tamoxifen and cheinotherapy for lymph node-negative,estrogen receptor-positive breast cancer. J Natl Cancer Inst. 1997 Nov 19;89(22):1673-82. | CrossRef | PubMed |Pritchard KI, Paterson AH, Fine S, Paul NA, Zee B, Shepherd LE, et al. Randomized trial of cyclophosphamide, methotrexate and fluorouracil chemotherapy added to tamoxifen as adjuvant therapy in postmenopausal women with node positive, estrogen and/or progesterone receptor positive breast cancer: A report of the National Cancer Institute of Canada Clinical Trials Group Breast Cancer Site Group. J Clin Oncol. 1997 Jun;15(6):2302-11. | PubMed |Castiglione-Gertsch M, Price KN, Nasi ML, et al. Is the addition of adjuvant chemotherapy always necessary in node negative postmenopausal breast cancer patients who receive tamoxifen? First results of IBCSG trial IX. Proc Am Soc Clin Oncol 2000; 19: 73a (abst.281). Fisher B, Redmond C, Wickerham DL, Bowman D, Schipper H, Wolmark N, et al. Doxorubicin containing regimens for the treatment of Stage II breast cancer. The National Surgical Adjuvant Breast and Bowel Project experience. J Clin Oncol. 1989 May;7(5):572-82. | PubMed |Misset JL, di Palma M, Delgado M, Plagne R, Chollet P, Fumoleau P, et al. Adjuvant treatment of node-positive breast cancer with oyclophosphamide, doxorubicin, fluorouracil and vincristine versus cyclophosphamide, methotrexate and fluorouracil. Final report after a 16 year median follow-up duration. J Clin Oncol. 1996 Apr;14(4):1136-45. | PubMed |Tormey DC, Gray R, Abeloff MD, Roseman DL, Gilchrist KW, Barylak EJ, et al. Adjuvant therapy with a doxorubicin regimen and long-term tamoxifen in premenopausal breast cancer patients. An Eastern Cooperative Oncology Group trial. J Clin Oncol. 1992 Dec;10(12):1848-56. | PubMed |Coombes RC, Bliss JM, Wils J, Morvan F, EspiÈ M, Amadori D, et al. Adjuvant cyclophosphamide, methotrexate and fluorouracil versus fluorouracil, epirubicin and cyclophosphamide chemotherapy in premenopausal woman with axillary node-positive operable breast cancer: Results of a randomized trial. J Clin Oncol. 1996 Jan;14(1):35-45. | PubMed |Lohrisch C, Di Leo A, Piccart MJ. Optimal adjuvant cytotoxic therapy for breast cancer. The Breast 2001;10 (Suppl 3):106-113. Basser RL. Optimal dose of chemotherapy in adjuvant treatment of breast cancer. The Breast 2001; 10 (Suppl 3): 96ó100. Colleoni M,Gelber RD, Gelber S,Castiglione-Gertsoh M,Coates AS,Goldhirsch A: ìHow to improve timing and duration of adjuvant chemotherapy. The Breast 2001;10 (Suppl 3):101-105. Hryniuk W, Levine MN. Analysis of dose Intensity for adjuvant chemotherapy trials in Stage II breast cancer. J Clin Oncol. 1986 Aug;4(8):1162-70. | PubMed |Budman DR, Berry DA, Cirrincione CT, Henderson IC, Wood WC, Weiss RB, et al. Dose and dose intensity as determinants of outcome in the adjuvant treatment of breast cancer. J Natl Cancer Inst. 1998 Aug 19;90(16):1205-11. | CrossRef | PubMed |Bonneterre J, Roche H,Bremond A et al. Results of a randomized trial of adjuvant chemotherapy with FEC 50 vs FEC 100 in high risk node-positive breast cancer patients. Proc Am Soc Clin Oncol 1998; 17:124a (abst 473). Henderson IC, Beny D, Demetri G et al. Improved disease-free and overall sur vival from the addition of sequential paclitaxel but not from the escalation of doxorubicin dose level in the adjuvant chemotherapy of patients with node positive primary breast cancer. Proc Am Soc Clin Oncol 1998; 17:101a (abst 390™) Fisher B, Anderson S, Wickerham DL, DeCillis A, Dimitrov N, Mamounas E, et al. Increased intensification and total dose of cyclophosphamide in a doxorubicin-cyclophosphamicle regimen for the treatment of primary breast cancer. Findings from National Surgical Adjuvant Breast and Bowel Project B-22. J Clin Oncol. 1997 May;15(5):1858-69. | PubMed |Fisher B, Anderson S, DeCillis A, Dimitrov N, Atkins JN, Fehrenbacher L, et al. Further evaluation of intensified and increased total dose of cyclophosphamide for the treatment of primary breast cancer: Findings from National Surgical Adjuvant Breast and Bowel Project B-25. J Clin Oncol. 1999 Nov;17(11):3374-88. | PubMed |Hudis C, Seidman A, Baselga J, Raptis G, Lebwohl D, Gilewski T, et al. Sequential dose-dense doxorubicin, paclitaxel and cyclophosphamide for resectable high-risk breast cancer: Feasibility and efficacy. J Clin Oncol. 1999 Jan;17(1):93-100. | PubMed |Bonadonna G,Zambetti M,Valagusa P. Sequential or alternating doxorubicin and CMF regimens in breast cancer with more than three positive nodes. Ten-yearsí results. JAMA. 1995 Feb 15;273(7):542-7. | CrossRef | PubMed |Muss HB, Thor AD, Berry DA, Kute T, Liu ET, Koerner F, et al. c-erb B-2 expression and response to adjuvant chernotherapy in women with node-positive early breast cancer. N Engl J Med. 1994 May 5;330(18):1260-6. | CrossRef | PubMed |Thor AD, Berry DA, Budman DR, Muss HB, Kute T, Henderson IC, et al. erb B-2, p53 and efficacy of adjuvant therapy in lymph node positive breast cancer. J Natl Cancer Inst. 1998 Sep 16;90(18):1346-60. | CrossRef | PubMed |Paik S, Bryant J, Park C, Fisher B, Tan-Chiu E, Hyams D, et al. erb B-2 and response to doxoruticin in pacients with axillary lymph node-positive, hormone receptor-negative breast cancer J Natl Cancer Inst. 1998 Sep 16;90(18):1361-70. | CrossRef | PubMed |Berry DA, Thor A, Cirrincione C, et al. Scientific inference and predictions; multiplicities and convincing stories: A case study in breast cancer therapy En: Statistics 5, Oxford UK. Oxford University Press. 1996, p 45ó67. Paik S, Bryant J,Tan-Chiu E, et al. HER 2 and choice of adjuvant chemotherapy for invasive breast cancer. National Surgical Adjuvant Breast and Powel Project Protocol B-15 J Nat Cancer Inst 2000;92: 1991-1998. Gusterson BA, Gelber RD, Goldhirsch A, Price KN, S‰ve-Sˆderborgh J, Anbazhagan R, et al. Prognostic importance of c-erb B-2 expression in breast cancer. J Clin Oncol. 1992 Jul;10(7):1049-56. | PubMed |Barnes DM, Smith S, Rubens RD. The relationship between outcome following adjuvant CMF and the presence of estrogen receptor and c-erb B-2 protein in 277 women with primary breast cancer. Breast Cancer Res Treat 1997;46:65 (abst 257). Phase III randomized study of doxorubicin and cyclophosphamide followed by paclitaxel with or without trastuzuinab (Herceptin) in women with node positive breast cancer that overexpresses HER 2. National Surgical Adjuvant Breast and Bowel Project B-31. BCIRG 006: A multicenter phase III randomized trial comparing docetaxel in combination with doxorubicin and cyclophosphamide (TAC) versus doxorubiciri and cyclophosphamide followed by docetaxel and Herceptin (AC--TH) versus doce- taxel and platinum salt and Herceptin (TCH) in the treatment of node positive and high risk node negative adjuvant patients with operable breast cancer who overexpress HER 2 NEU. Breast Cancer International Research Group 006. Perez EA. Adjuvant anti-HER 2 monoclonal antibody therapy - ready for breast cancer? The Breast 2001; 10 (Suppl 3 ):161ó163. Davidson NE,Wolff AC. The use of anthracyclines and taxanes for adjuvant therapy of breast cancer. The Breast 2001:10 (Suppl 3): 90-95. Henderson IC: CALGB ria l9344NIH Dc an Adjuvant Therapy for Breast Cancer 2000 ; Bethesda,MD.USA. Adjuvant therapy for breast cancer. NIH Consens Statement. 2000 Nov 1-3;17(4):1-35.
11512506 Mamounas EF. Evaluating the use of paclitaxel following doxorubicin/cyclophosphamide in patients with breast cancer and positive axillary rodes NSABP B-28 protocol. NIH CDC on adjuvant therapy for breast cancer, 2000; Bethesda, MD.USA. Thomas E, Buzdar A, Theriault R et al. Role of paclitaxel in adjuvant therapy of operable breast cancer: Preliminary results of prospective randomized clinical trial. Proc Am Soc Clin Oncol. 2000;19:74 A (abst 285) BCIRG 001/TAX 316: A multicenter phase III randomized trial comparing docetaxel in combination with doxorubicin and cyclophosphamide (TAC) versus 5-Fluorouracil in combination with doxorubicin and cyclophosphamide (FAC) as adjuvant treatment of operable breast cancer patients with positive axillary Lymph nodes. Breast Cancer International Research Group TAX 316 protocol. Faculty members: ìOngoing trials of polychemotherapy for nodeónegative disease. En: Prognosis and treatment of node negative breast cancer. . Philadelphia, PA. USA, Ed.CE Gilmore, Phillips Group Oncology Comunications Co, 2001:p 18-19. Peters WP, Roaner G,Vredenburgh J et al. A prospective randomized camparison of two doses of combination alkylating agents as consolidation after CAF in high-risk primary breast cancer involving ten or more axillary lymph nodes: preliminary results of CALGB 9082/SWOG 9114/NCIC NA-13. Proc Am Soc Clin Oncol 1999:18: 1™. (abstr). Bergh J, Wiklund T, Erikstein B, Lidbrink E, Lindman H, Malmstrˆm P, et al. Tailored fluorauracil, epirubicin, and cyclophosphamide compared with marrow-supported high-dose chemotherapy as adjuvant treatment for high-risk breast cancer: A randomised trial. Scandinavian Breast Group 9401 study. Lancet. 2000 Oct 21;356(9239):1384-91. | CrossRef | PubMed |Rodenhius S, Bontembal M, Beex L. et al. Randomized phase III study of high-dose chemotherapy with cyclophasphamide, thiotepa, and carboplatin in operable Breast cancer with 4 or more axillary lymph nodes. Proc Am Soc Clin Oncol 2000;19: 74a (abstr 286). Rodenhuis S, Huitema AD, van Dam FS, de Vries EG, Beijnen JH. High dose chemotherapy with peripheral blood progenitor cell transplantation in the adjuvant treatment of breast Cancer. Cancer J. 2000 Apr;6 Suppl 2:S125-30. | PubMed |Rodenhuis S, Richel DJ, van der Wall E, Schornagel JH, Baars JW, Koning CC, et al. Randomised trial of highdose chemotherapy and haemopoietic progenitor-cell support in operable breast cancer with extensive axillary iymph-node involvement. Lancet. 1998 Aug 15;352(9127):515-21. | CrossRef | PubMed |Hortobagyi GN, Buzdar AU, Theriault RL, Valero V, Frye D, Booser DJ, et al. Randomized trial of highdose chemotherapy and blood cell autografts for high-risk primary breast carcinoma. J Natl Cancer Inst. 2000 Feb 2;92(3):225-33. | CrossRef | PubMed |Mouridsen H,Andersen J,Anderson M et al. Adjuvant anthracycline in breast cancer. Improved outcome in premenopausal patients following substitution of methotrexate in the CMP combination with epirubicin. Proc Am Soc Clin Oncol 1999;18:68a (Abst 254). 






 Estudios originales
Estudios originales