Revista BiomÚdica Revisada Por Pares

 Para Descargar PDF debe Abrir sesiˇn.
Para Descargar PDF debe Abrir sesiˇn.
Palabras clave: hypertension, aged, healthy lifestyle, healthy diet, exercise, culture, primary healthcare
OBJECTIVE
To identify resources of the municipality of Sopˇ-Cundinamarca, Colombia, that are also opportunities to strengthen the development of an educational strategy that promotes healthy habits (healthy diet and exercise) as part of the comprehensive management of hypertension in the elderly.
METHODS
A qualitative study of a participatory-action research initiative in the Community Day Center of Sopˇ in the second semester of 2015. It was developed in three stages: first, a community diagnosis showed the need to integrate the culture, traditions and resources of the municipality as inputs that allow the adherence of healthy styles by the elderly for the control of hypertension; in the second stage, a work plan was established based on actions provided by the community; and in the third stage, we reflected on the results.
RESULTS
An effective and sustainable intervention for the elderly can be achieved through the following activities: appropriation of the agricultural resources, the strengthening of dance as a form of exercise, use of motivational strategies, support of institutions that work with the welfare of the elderly, and the empowerment of facilitators.
CONCLUSIONS
Interventions aimed at supporting the adherence of healthy lifestyles to the elderly should include and preserve the context of the community of which they are part, where community resources are the inputs that allow health promotion.
Colombia is a country with a significant change in the population pyramid, since life expectancy at the national level has increased and thus, aging has increased. This results in a high prevalence of chronic diseases in the elderly, highlighting hypertension (HTN) as the most prevalent disease in the national territory [1]. Therefore, it is necessary to carry out studies oriented to the development of strategies that promote well-being in the elderly and thus allow the promotion of health in this population group [2].
Therefore, it is necessary to broaden the picture and recognize that therapeutic adherence remains an obstacle that does not allow improvements in the health and quality of life of the people. According to data from the World Health Organization (WHO), adherence rates to treatments for chronic diseases are around 50% in the developed countries, a fact that allows us to classify adherence as a global problem of great magnitude [3].
We understand therapeutic adherence as the extent to which the patient accepts the rules or advice given by the health professional, from the point of view of habits or lifestyle, as well as the prescribed pharmacological treatment itself. It also expresses the degree of coincidence between the orientations given by the health professional and those followed by the patient, after a decision fully reasoned by the latter [3].
Additionally, adherence problems are always present, regardless of the disease, patient type, demographic group, or socioeconomic level [4]. In the case of hypertension, 7.1% of patients quit the medications indicated by the family doctor and 22.4% in the case of specialists. At the same time, it is noteworthy that adherence to a healthy diet is lower with respect to medication, being 59% and 79.4%, respectively [4]. Similarly, there is a direct relationship between adherence and a favorable course of the disease, or less deterioration [5]. In the case of patients with hypertension, adequate adherence to antihypertensive treatment reduces the risk of stroke by 8-9% and the risk of death by 7% [6].
These data are congruent with the need to implement strategies aimed at improving adherence in aspects related to living habits (healthy diet and exercise) that are more difficult to modify through educational strategies, in comparison with those linked to simpler changes (for example, taking a medication over a short period of time is easier than changing dietary habits) [4].
On the other hand, it is pertinent to approach hypertension from a holistic perspective, analyzing the patient as an active person in a society and a community, where traditions and behaviors are demarcated in different aspects, including health care [7]. The participatory-action research (PAR) allows this approach, through the exchange of knowledge between the researcher and a specific population. By means of collective work, it is possible to characterize the community and establish those situations that require a process of transformation. Likewise, this method can answer questions such as this: why do older adults have low adherence to healthy habits (healthy diet and exercise)? Even more, it allows to generate improvement plans from resources and community actions [8].
One of the reasons for a low adherence to healthy habits is the absence of educational programs that integrate the cultural context, the traditions and the specific motivations of each community. Together with behaviors of healthy life, this integration would improve the management of chronic entities such as hypertension and the control of its complications [9],[10].
According to the above, an educational intervention should allow the active participation of patients, increasing knowledge, monitoring and control of the disease. Taking into account that lifestyle interventions are as effective as pharmacological management, besides having social and health significance [11].
In the specific case of the elderly, the intervention program should be based on strategies that have been a differentiator in the promotion of their health. For the case of Colombia, Adult Daycare Centers, are an example of this issue. These institutions are dedicated to the care, integral well-being and social assistance of older adults, providing their services during daytime hours, being a social strategy on which the National Government plan bets [12]. In addition, articulating the different people who are caring for the older adult improves the outcome of this type of interventions [13]. In this way, by merging the culture with the available resources of the community, as the human resources, it is possible to impact on the health of the older adult, starting from an approach from primary health care (PHC) [14].
Considering the above, we decided to understand the cultural context of the municipality of Sopó-Cundinamarca (Colombia), with the objective of identifying the resources of this municipality, as opportunities to strengthen for the development of an educational strategy that promotes healthy habits (healthy diet and exercise) as part of the comprehensive management of hypertension in the elderly.
During the second half of 2015, a qualitative study, participatory-action research type, was carried out with a working group of 121 seniors between the ages of 60 and 90, who attend Adult Daycare Center: “Memories that build”. There, they are part of the group “Wisdom´s White hair”, of the municipality of Sopó. The five professionals who work with them (gerontologist, graduate in physical education, psychologist, nutritionist and teacher of crafts) were also included in the work. These professionals collaborated and actively promoted this project, so they were called facilitators.
The selection of the population was made for convenience, choosing the group of older adults more active and willing to participate in the process, the facilitators working with them were also involved.
Thus, the participating population met the following inclusion criteria: to be older adults in the range of 60 to 90 years, members and participants in the activities of Adult Daycare Center; in the case of the facilitators, all participated because they were in daily and continuous contact with the elderly. Each of them gave their consent to participate after an explanation of the project.
The research work was developed through three stages. In the first, an approach and knowledge of the community is generated, in order to achieve the community diagnosis. In the second, the work plan is established where actions based on the strategies was provided by the community. Finally, in the third stage, improvement and reflection on some aspects are undertaken, based on the results of the activities carried out before.
As part of the participatory process, participants are the owners of the research. In the same way, both the elderly and the facilitators discussed and signed a document called "agreement of wills", where the commitments and ethical elements between the parties are mentioned. From this “agreement of will”, a contract between the University of La Sabana and the municipal administration of Mayor of Sopó derived, the realization of which was reviewed by the committees and dependencies of both entities for approval and signature.
First stage: community diagnosis
In the first instance, the Adult Daycare Center was contacted to generate a rapprochement and knowledge of the community. Subsequently, a community diagnosis was made corresponding to the elderly population. This included elements from primary sources (surveys, semi-structured interviews, discussion groups, and observations) and secondary sources (documentary revision, normative revision, review of the literature and statistics), thus identifying the main problems and health needs of the community.
This information was consolidated in a list identifying different problems related to health. Afterwards, the prioritization process was made (consultation and discussion with the community) using the Hanlon method [15]. Each of the elements is discussed in a concerted way, and the community diagnosis is achieved jointly: the older adults of Adult Daycare Center in Sopó don’t appropriate (understand and apply) healthy lifestyles (healthy diet and exercise) for the integral management of hypertension.
Second stage: work plan
Once the community diagnosis was established, a proposal for improvement was completed. For this, a matrix was made, supported by a literature review concerning the problem, which included the objective of the present work. From this, some achievements (specific goals) are established to reach the objective; therefore, these achievements are carried out from the development of concrete activities, which are evaluated by means of a verifier. This verifier allows evaluating the fulfillment of the goal, for what is called “indicator”.
The exploration of the knowledge that the elders and the facilitators had on hypertension, was carried out through he application of a semi structured interview, which contained questions about risk factors, clinical manifestations, complications, and treatment. This section focused on healthy patterns (healthy diet and exercise), how they were implemented, and what were the reasons for poor adherence to them.
In turn, the community was asked about strategies that were to their liking and interest, which promote healthy habits in the elderly. In this way, the activities were developed from traditional games. In addition, videos of their authorship related to hypertension were projected, and spaces were created for the community to elaborate its own didactic material from the activities. Likewise, with the facilitators, training and reflection forums were held on their role in relation to the elderly.
In each of the activities, home works were assigned to the elderly from the knowledge acquired, so it could be diffused in their homes. Likewise, each activity underwent a process of evaluation, socialization and validation of the obtained data, through interviews, surveys or observation.
Third stage: codification of information
The information for each of the activities was manually collected and subsequently transcribed into a digital field diary. Then it was systematized and analyzed using matrices of categories and subcategories according to the objective and achieved accomplishments. The coding process was developed in two phases: the first involved the identification of early work codes and emerging categories. In the second instance, it was verified that the coding process had been performed correctly, the community being the evaluators of the data obtained, who validated the information. Throughout the systematization, each category was in depth defined and analyzed. Likewise, during the analysis, we went deeper into the connection relationships between categories. Both the systematization and the analysis process were developed simultaneously, through the repeated reflection (re-signification of the practice) of the researchers on the obtained data.
This article presents the results in categories that allow an approach to the hypertensive elderly and its adoption of healthy guidelines from the appropriation of the resources of the municipality. These categories are presented in Table 1.
Table 1. Categories of results.
Characterization of the community and its experience in the Adult Daycare Center
We worked with 121 older adults, of whom 64% were women and 36% were men. All were in an age range of 60-90 years; 35% in the range of 71-80 years; 33% in 60-70 years; and 32% in 81-90 years.
Most of them (65%) were not natives of the municipality of Sopó but of surrounding municipalities, and have lived in Sopó for around the last 20 years of their life, after completing their work period. They are homogeneously distributed between rural and urban areas, all the older adults are part of the socioeconomic levels 1 and 2 which are the lowest levels given by their situation of poverty and vulnerability [16].
In relation to the structure of the home, the majority live with their children and grandchildren. In general, the elderly showed that their economic situation allows them to meet their basic needs, thanks to the financial support of their children and the subsidy offered by the municipal government.
About 50% of older adults had been part of the Adult Daycare Center for approximately 10 years and attend two days a week, Tuesday in the morning and Wednesday in the afternoon. There are activities such as personal growth workshops and social relationships, educational outings, cultural dance-theater-music meetings, spaces aimed at physical activity and body care. These activities allow the elderly to feel recognized, and above all to live aging as a natural process with quality of life, mitigating their conditions of vulnerability.
“In the Adult Daycare Center I have learned to be sociable, to learn from other people, to take care of my health, to know my limits, to see others alike, to be tolerant, to be supportive, to recognize the importance of medicines, to make crafts such as knitting, painting, stained glass; learning to do physical exercise, and in turn I have learned about common diseases, and their care”.
“Live a little better”.
Of the 121 older adults who participated in the project, 27 received the initial and final surveys, since they participated in all the developed activities, maintaining a continuum of the process.
Older adults interact at Adult Daycare Center with five facilitators, who have been working with them for four years, in order to promote health, disease prevention, and alterations presented by the aging process, thus optimizing their quality of life. Four of the facilitators are university graduates, and one has a degree in technology. None of them are hypertensive, however they have family experiences about the behavior of the disease and its care.
“Our goal is to ensure that older adults who belong to the Adult Daycare Center improve their quality of life through healthy lifestyles, health promotion, disease prevention and mitigating the alterations of aging”.
Based on shared experiences at the Adult Daycare Center between seniors and facilitators, the elderly perceive the Adult Daycare Center as a wellness area that offers them quality of life based on the activities carried out and the treatment they are offered.
“In Adult Daycare Center I feel very good because they care about the welfare of us”.
“When we arrived here we forgot about the problems of the house”.
“We can share with other people”. “It is the reason of my life”.
“It removes negative thoughts and sorrows”.
“A lot of love is offered here to all people from the administrator, the teachers are very sensitive and loving, they treat us very well, they are educated, and they are a support”.
Knowledge of older adults about hypertension
Hypertension is one of the most prevalent diseases in the elderly in the Adult Daycare Center, most of them diagnosed more than 10 years ago. They know it is a chronic disease, although they do not know the exact values of hypertension. They recognize that this entity compromises organs like eyes, brain, heart and kidney. They also know that hypertension combined with risk factors such as obesity, hypercholesterolemia, smoking, and alcoholism increases the risk of cardiovascular disease.
“Most of us here have hypertension”.
“It affects the head and the thought. It makes you sick, it makes you dizzy. It gives you a more serious problem like a heart attack, thrombosis, stroke”.
“One is left as a fool, and with half-paralyzed body”.
Users are aware that hypertension is not only managed with medications, since they recognize the importance of a healthy diet in the hypertensive patient, which should be abundant in vegetables and fruits, low in fat, and restriction in salt consumption. However, they do not know the impact of the sodium in hypertension, and they don't know what foods this element is in. Additionally, given that in this pathology, certain care must be taken with food, they label this disease as the one that takes away everything.
“We can not eat sweet, no alcohol, no fat, no flour, no salt, no snacks or sausage”.
“Being hypertensive means we are banned from everything, no fats and no alcohol. And you cannot eat salt or sweet”.
In addition, they identify that continuous physical activity is one of the components within the integral management of this entity. They know that people who are overweight or obese when they lose weight improve the control of hypertension. However, they present shortcomings in how to perform physical activity and the duration of it to be beneficial.
“With exercise one relaxes, sweats, and takes away all worry”.
“Physical activity is okay for high blood pressure, for good weight, for health and for good circulation”.
The facilitator is a reference of knowledge of hypertension and healthy habits
Regarding the facilitators, they know about hypertension from the experiences with their relatives, they recognize it is due to vascular resistance to the blood flow, generating an increase in systolic blood pressure (SBP) or diastolic blood pressure (DBP), and secondary pathological changes.
“It is the increase of diastole and systole, is the resistance of the arteries to the passage of blood”.
“There is no care of the arteries, for example the fat breaks off and forms clots, which break off and hamper”.
They relate this entity to bad habits such as diet rich in carbohydrates, fats and salt, high consumption of alcohol and tobacco, and elevated levels of serum cholesterol, which should be reduced in the hypertensive patient. In turn, they identify sodium as a detrimental element to the control of hypertension, and throughout the project they learned to identify foods rich in this element.
“You should avoid alcohol, cigarette, fats, greaves, sweets, packets. Older adults do not know which foods contain more salt or sodium”.
“I've heard that sodium is bad for people with high blood pressure although I do not know what it does in the body”.
“I learned that sodium is in canned food, junk food, sausage, sauces, and everything that has preservatives, and you should not eat that because it is bad and more for hypertension”.
In addition, they know about the complications of the disease, and consider them as fatal outcomes due to the impairment of functionality. Within the main complications they recognize acute myocardial infarction (AMI) and stroke.
“One of the complications is thrombosis, for example, Mr. Sarmiento of the afternoon group has half-body paralysis, and also has hypertension”.
“An aunt of mine has had hypertension for years, she did not take care of herself, and she recently had a heart attack”.
They recognize that both the onset of illness and complications can be avoided by incorporating healthy habits into their lives.
They identify the benefits of performing physical activity for different systems of the human body, and have observed how people's lives change.
“It should be done 20-40 minutes, depending on age and physical condition. Mild to moderate intensity. Three times a week”.
“The activities they can perform are walking, stretching, strengthening motor skills, strength, elasticity, proper breathing according to the pathologies. You have to adapt the exercises to the capacities they have”.
“Increases oxygenation, strengthens muscles, respiratory part, bone and brain. Here we can see the change in the people who perform physical activity, a man used a walking stick to carry out all the activities, after I arrive here, I leave the walking stick, and now walks through the town without the help of the walking stick”.
Resuming traditions and customs as a source of knowledge in healthy guidelines
The majority of older adults who were not native to the municipality of Sopó were unaware of the food they grow there. This knowledge was gradually appropriated throughout the project through the different activities. They had a great information about traditional foods that help in the control of hypertension, which was reinforced from the scientific knowledge about its benefits and properties for the control of this and other pathologies.
“Tangerine peel, lulo juice, not eating acid foods, drink enough water, aromatic, tree tomato juice, brevo, glass of water in the early morning, are good for hypertension”.
Taking into account that the interest of the community is focused on the recognition and appropriation of the resources offered by the municipality, a visit is made to the crops of the place, where they identified the foods that are grown there and design a list of them, later a review of the literature was made extracting the properties and benefits, noting that foods such as guatila, breva and chard exert an important control over blood pressure. In turn, there are grown other foods such as cherry tomato, auyama, celery, broccoli, zuchini, head onion, cauliflower, melissa and lettuce, which in addition to acting on the control of blood pressure, help in the maintenance of health.
Once the elderly identified these foods and their benefits in the control of hypertension, they encouraged their family members to consume them more frequently at home. It is noteworthy that they are amazed by the easy access they have to these foods, since being grown in the municipality, its cost is affordable for them. They also identified that excessive and periodic consumption of foods rich in carbohydrates and fats is detrimental to health, and they learned that sodium is a mineral that should be restricted in their diet, but, more than this, they learned to identify foods that contain it.
“Of course! After that I went down as far as possible to the salt, I lowered the fried, the flours, I had to quit smoking, I stopped drinking, I had to exercise, I had to eat more salads and vegetables”.
“I knew that guatila and brevo are good for hypertension, but now I learned more, and I met others who also serve, the melissa, the zuchini, which I love so much, the chard, Now our plate will be full of vegetables”.
“All in the house we eat more vegetables and we lower the flours, for example we replace the potato by the guatila”.
“I would like to eat fish every day, but money does not reach me, instead if I can buy the vegetables that are grown here and help me for blood pressure”.
“You do not have to eat canned goods, packets, sausages, junk food because all that brings sodium and is bad for your health”.
On the other hand, physical activity as a healthy pattern was also reinforced, starting from the fact that the elderly in the Adult Daycare Center know the importance of physical activity to maintain an active and healthy life. They recognize the proper exercises that they should perform according to their physical condition such as aerobics, walking, stretching and balance exercises. Each of these exercises are put into practice in Adult Daycare Center and in their daily life, mainly aerobic exercises like dancing and the daily walk.
“In the Adult Daycare Center we make walks, warm-ups, stretching exercises, dances, exercises with wheels, sticks, and aerobics”.
“We love dancing, we're glad, it gives us energy, it's the best exercise”.
“Every day I walk through the village, all over the hill, I visit my friends and I feel energetic. I think this has been what has helped me stay healthy”.
It should be taken into account that older adults present certain limitations to perform physical activity, such as comorbidities, mainly osteoarticular, and poor physical condition.
Methods of motivation to the community
Both older adults and facilitators through videos of their authorship on hypertension complications, learned about the importance of incorporating healthy habits into their lives, and extend this invitation to the community. They invite young people to take care of themselves at an early age, and thus prevent the onset of the disease and the development of complications. And if these are already present, they indicate following the doctor's recommendations.
“After the paralysis I have always told them not to eat so salty, do not eat so many flours, and try to do some exercise ... to take care as much as you can, because life is in taking care of one”.
“I've known this person from the video for a long time, he ate a lot of fat, smoked and drank too much, this happened on a work day, near the river bank and we all thought he was dead, but then we saw that half of the body was paralyzed. This story is very important because it helps us realize that we must take care of food and exercise, to avoid being sick in the future”.
“I recommend to my colleagues at the Adult Daycare Center and not only them but all people, to stop eating too much fat and flour, because we are addicts, this is very important. Two years ago I had a heart attack, had an open heart surgery and I lasted about six months recovering, for a long time I could not play ping-pong and micro football, so after a long time I was able to resume the activities that I liked to do”.
“The doctor told me to walk an hour a day, besides taking care of the food, if I ate potatoes, I could not eat rice”.
“In working with the grandparents, I have learned that you have to take care of yourself since you are young, because you see cases where they look bad because of the complications. One learns daily with them, that if they had taken care they would not be in the conditions they are now, and it is unfortunate to see that from one moment to another they can have a heart attack and it is because they have not taken care of their body, nor in the diet”.
Similarly, older adults reflected on the importance of incorporating into their lives healthy patterns from projections in the future, (how they might look in five years). Everyone agrees that they want to be functional, without depending on anyone, to be able to continue with their activities, to share with their families. The factor that impacted them most was not being able to share with their grandchildren, secondary to a complication of hypertension, such as an acute myocardial infarct or stroke, and this motivates them to take care of their health.
“Of course I see myself walking, doing my jobs home, I do not want to be a nuisance. I want to see my granddaughter graduate and I would not be able to do it, that's why I know I should eat well and take care of myself, if it's not too late".
"I do not want to be bad for my family, I want to be with my daughters and children, I'm afraid of paralysis and not being able to play with them ... that's where you realize that everything you tell us is true about giving up eating fries, potatoes, rice and move to not get fat”.
The role of the facilitator in maintaining health
Facilitators are perceived by older adults as authority on health issues, as in the case of hypertension, this allows seniors to resolve doubts on the subject with facilitators, since they explain to them that it is the disease, its complications, and healthy habits.
“Teachers tell us about hypertension, explain to us what the disease is and how to take care of ourselves ... That's why I constantly ask them about whether I have blood pressure well, if I am well, my controls, and they are pending”.
In relation to healthy habits, the facilitators are promoters of the theme, through the activities they develop with them, teach them about key points, such as the importance of a balanced diet, how to perform adequate stretching, aerobic exercises and the time required.
“They see us as their family, and that is why we must watch over them, teach them to take care of themselves, in activities beyond the game, the important thing is for them to learn about nutritious foods, their benefits, so that they take care of themselves”.
Likewise, the facilitators care about the nutrition of the elderly, for example the snacks that are provided at the Adult Daycare Center are prepared by the nutritionist, who is concerned with providing a balanced dish with an adequate nutritional content. From this simple practice adults come to their homes motivated and prepare healthy dishes for lunch and dinner.
“Here they give us healthy snacks, they take care of us a lot, our nutritionist is aware of that ... and I try to be judicious also in the house”.
Facilitators through training and reflection forums recognized the impact they exert on older adults and how they can instill in them healthy guidelines for the care of their health. Since then, they couple the learned wisdom to the different activities they develop with the elderly.
“We learned that in the activities we can teach them more things, for example they loved learning about the food grown here and its benefits with the game of “bolirana” ... It is a very good strategy and we will implement it from now on”.
They also care about giving continuity to each of the lessons learned, so in each activity they develop, they take back the previous knowledge that was taught to reinforce them and integrate them with the new themes.
“So in all activities we are reminding them of what they have learned, and so they are not forgotten”.
The adoption of healthy habits such as food and physical activity has become one of the most effective strategies in the prevention of cardiovascular complications secondary to hypertension and also as a protective factor against other entities and other benefits widely described in the scientific literature [17]. However, achieving adherence to healthy habits means a challenge for today's society. This study is pertinent to this call, since it elucidates some of the essential tools to guide and complement the adherence strategies of healthy guidelines in the hypertensive elderly population, based on an educational proposal that integrates the cultural resources, that is to say the environment and the traditions, and adapts them to the own characteristics of the community of Sopó.
The findings corroborate the importance of implementing lifestyle interventions (healthy diet and exercise) and combining them with pharmacological management, thus achieving a better control of blood pressure [18]. In turn, we describe the causes that do not allow this binomial, such as cultural beliefs, and barriers to access both pharmacological management and healthy lifestyles [19].
The level of knowledge of older adults about healthy patterns is acceptable, which is consistent with the literature [20]. Nevertheless, it is necessary to establish an educational program with cultural sensitivity that focuses on the adherence of style changes of life and medication [21].
Likewise, it was identified that the elderly recognize the hypertension, its risk factors, and complications, the latter being the ones who they are most afraid of, because of the functional sequels it leaves. For this reason, we consider essential to carry a comprehensive treatment: drugs, food and physical activity. This knowledge is acquired from the consultation with his doctor, and the lived experiences of relatives or near beings, data observed in the literature [20].
It was recognized that the dynamics of culture, traditions, and beliefs of older adults are strategies that make a difference in the adoption of healthy guidelines [7], since this allows their identity to be recognized and do not feel violated, and so they recognize their own resources, which are nothing alien to them, and which provide great benefits to their health [9].
Older adults have had an important contact with agricultural life, so they prefer foods that are grown than those that are processed and industrialized, and more if food is produced in their region. This is a topic that captures all their interest [21], which allowed the creation of an educational tool for health promotion, which is easily accessible for the implementation of healthy eating for the hypertensive patient [22].
On the other hand, the adoption of strategies as traditional games, is an instrument that generates confidence and interest for learning [23]. Through dynamics full of tradition and culture, older adults reinforced their knowledge about agricultural foods in the municipality of Sopó, which helps them to control hypertension, especially guatila (Sechium edule) and brevo (Ficus carica).
It is necessary to highlight that older adults already had an important ancestral knowledge, which allowed them to know that these foods help in the control of blood pressure, but they did not know the mechanism that generates this effect. Guatila is a natural resource for the control of blood pressure by its hydro alcoholic extract which has been used in murine models and it has been observed that it decreases up to 30 mmHg approximately the blood pressure [24]. In turn, brevo is a fruit with cardiovascular activity, which has been empirically used as a traditional herbal medicine for the treatment of hypertension and other cardiovascular diseases, a dose of 1,000 mg / kg of its extract significantly decreases blood pressure, exerting an antihypertensive effect, so far are results in mice [25]. In this way, it is made clear that the ancestral knowledge possessed by older adults represents a great wealth of knowledge, and which cannot be disarticulated from healthy practices, on the contrary must be integrated harmoniously to these, making it clear that this is one of the fundamental pillars in the promotion of health, and that allows this to become facts.
It is noteworthy that, being foods grown in the municipality, they have a low cost, so they are easily accessible to the population. Since within the barriers for the adherence to the care of hypertension, the economic factor is found, this is why those who do not have the resources to access a healthy diet, consider it a high-cost pattern [26].
Similarly, older adults learned that dancing is a healthy pattern that allows them to perform physical activity, which provides them with great benefits for the care of their health and also comforts them [27]. Dancing is an activity well rooted in the national territory, since it is part of the identity and the sense of belonging. Therefore, the older adults demonstrate great passion for the dance, because from sounds of cumbia, corridors, and joropos, which are part of their roots, they feel identified and motivated, through this cultural instrument, to perform physical activity.
These practices of incorporating traditional dances of a specific region in the management of hypertension are as effective as other physical activities, since they reduce blood pressure, a fact that has been described in the literature [28]. In addition, it is an activity they can adapt to the osteoarticular comorbidities that so much afflict them, and that many times is the great impediment to physical activity. For this reason, dancing is one of their greatest incentives [29].
The older adult is identified in all the communities as the one that transmits knowledge to the different generations [30]. The Adult Daycare Center seniors shared what they had learned at home, promoting healthy habits in their family, changing the style of even the youngest of their grandchildren, who were motivated to consume more vegetables. This is how the older adult is a person who is a leader in families and who enjoys great respect for the experience and knowledge he possesses, so that important change interventions such as these can be achieved through them [31].
Another feature that helped raise awareness in the elderly were the autobiographical videos, where their colleagues, people they knew for a long time, tell their personal experience about some complication of hypertension, impacting them and leading them to reflect. This tool leaves in evidence that with activities like this one achieves greater impact than with an academic talk about complications of hypertension [32]. Likewise, reflecting on the future invites you to make a personal analysis of your self-care. Thus, these two activities are key guidelines, which when incorporated into health promotion strategies mark a differentiating element, which allows the older adult to understand that the main health monitor is him or herself, and that his or her future health depends on healthy habits they adopt today [33].
All this is achieved with the help of places that allow older adults to feel recognized. Strategies such as the Adult Daycare Center are sites that allow them to feel welcomed in society, a place where they can share their knowledge, share their fellows, and learn to live with their illnesses. For the older adult these spaces comforted them and they perceived them as a great support at this stage of their lives [34]. For these reasons, places like the Adult Daycare Center, are ideal places to promote health, since it is possible to reach a large number of elderly people in a quick and easy way, making them a means of facilitating the execution of actions promoted in primary health care. It is a vehicle that allows transcending in the promotion of health and disease prevention, based on shared knowledge and articulation, which allows the sustainability of the project [34]. This opens the way to encourage the creation and maintenance of institutions such as this, for the promotion of healthy communities.
Similarly, as the Adult Daycare Center is the intervention vehicle, facilitators are the guides, since they maintain a direct and close contact with the elderly, being a key part in the processes related to the older adult [35], since the older adult sees them as an authority of respect and knowledge, and also as a close person who watches for their care [36]. This makes it necessary to deepen the training of facilitators in health care strategies for the elderly [37].
Working with the older adult involves retaking their roots and adhering not only to them but to all those who are involved with them, mainly their caregivers. In addition, the different actors must rely on the cultural resources that the community offers them, from which interventions are adopted for the care of the elderly [38].
It should be noted that this study, using the participatory action research methodology, allowed for the exchange of knowledge between the researcher and the community, generating the transformation of a social reality, based on the intervention of a daily and immediate problem through concrete practices. In this way, the community became aware of its role in this process of transformation, through its practical knowledge, experiences and skills [8]. Even more, from these they built health. In addition, the participatory action research, beyond being a research method, allowed the promotion of Community-Oriented Primary Care (COPC), since when intervening a specific need of this community, the actions of the public health and the primary health care were integrated [39].
From this initiative an invitation is made to work for the elderly articulated and in team, where from them, as leaders of their community, caregivers, the strengthening of institutions caring for the elderly, the recognition of cultural resources, and the promotion of traditions; educational strategies are adopted, such as this one, that bets on the promotion of health with a focus from the primary health care, and that can also be replicable in other population groups with different community diagnoses.
From the editor
The authors originally submitted this article in Spanish and subsequently translated it into English. The Journal has not copyedited this version.
Ethical aspects
The Journal is aware that the study and its possible publication in a biomedical journal were approved by different committees (ethics, legal and academic) as part of the agreement between the University of La Sabana and the municipality of Sopó, Colombia.
Declaration of conflicts of interest
The authors have completed the ICMJE Conflict of Interest declaration form, and declare that they have not received funding for the report; have no financial relationships with organizations that might have an interest in the published article in the last three years; and have no other relationships or activities that could influence the published article. Forms can be requested by contacting the author responsible or the editorial management of the Journal.
Acknowledgements
We thank each of the members of Centro Día, Sopó, Cundinamarca (Colombia) for their willingness and support for the study.
Editor's note
The principal or responsible author asserts that this manuscript is an honest, accurate and transparent transcription of the study being reported; that no important aspects of the study have been omitted; and that discrepancies between the study results and those anticipated (if relevant) have been recorded and explained.
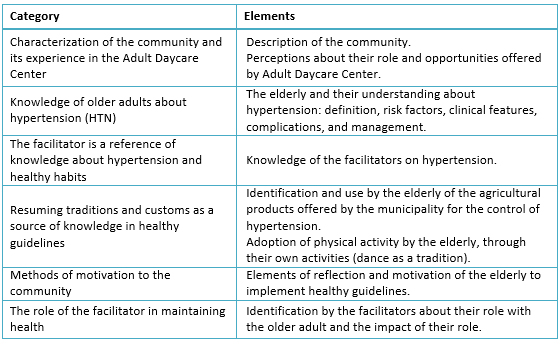 Table 1. Categories of results.
Table 1. Categories of results.
 Esta obra de Medwave estß bajo una licencia Creative Commons Atribuciˇn-NoComercial 3.0 Unported. Esta licencia permite el uso, distribuciˇn y reproducciˇn del artÝculo en cualquier medio, siempre y cuando se otorgue el crÚdito correspondiente al autor del artÝculo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave estß bajo una licencia Creative Commons Atribuciˇn-NoComercial 3.0 Unported. Esta licencia permite el uso, distribuciˇn y reproducciˇn del artÝculo en cualquier medio, siempre y cuando se otorgue el crÚdito correspondiente al autor del artÝculo y al medio en que se publica, en este caso, Medwave.
OBJECTIVE
To identify resources of the municipality of Sopˇ-Cundinamarca, Colombia, that are also opportunities to strengthen the development of an educational strategy that promotes healthy habits (healthy diet and exercise) as part of the comprehensive management of hypertension in the elderly.
METHODS
A qualitative study of a participatory-action research initiative in the Community Day Center of Sopˇ in the second semester of 2015. It was developed in three stages: first, a community diagnosis showed the need to integrate the culture, traditions and resources of the municipality as inputs that allow the adherence of healthy styles by the elderly for the control of hypertension; in the second stage, a work plan was established based on actions provided by the community; and in the third stage, we reflected on the results.
RESULTS
An effective and sustainable intervention for the elderly can be achieved through the following activities: appropriation of the agricultural resources, the strengthening of dance as a form of exercise, use of motivational strategies, support of institutions that work with the welfare of the elderly, and the empowerment of facilitators.
CONCLUSIONS
Interventions aimed at supporting the adherence of healthy lifestyles to the elderly should include and preserve the context of the community of which they are part, where community resources are the inputs that allow health promotion.
Autores:
MarÝa Carolina Lˇpez-Mateus[1], Erwin Hernando Hernßndez-Rincˇn[2], Camilo Alejandro Correal-Mu˝oz[2], Gina Paola Cadena-Buitrago[1], Ingrid Johanna Galvis-DÝaz[1], GÚnesis Esmeralda Romero-Prieto[1]
Citaciˇn: Lˇpez-Mateus MC, Hernßndez-Rincˇn EH, Correal-Mu˝oz CA, Cadena-Buitrago GP, Galvis-DÝaz IJ, Romero-Prieto GE. An educational strategy that promotes healthy habits in elderly people with hypertension in a municipality of Colombia: a participatory action research study. Medwave 2017 Sep-Oct;17(8):e7072 doi: 10.5867/medwave.2017.08.7072
Fecha de envÝo: 26/6/2017
Fecha de aceptaciˇn: 25/9/2017
Fecha de publicaciˇn: 30/10/2017
Origen: no solicitado
Tipo de revisiˇn: con revisiˇn por tres pares revisores externos, a doble ciego
Nos complace que usted tenga interÚs en comentar uno de nuestros artÝculos. Su comentario serß publicado inmediatamente. No obstante, Medwave se reserva el derecho a eliminarlo posteriormente si la direcciˇn editorial considera que su comentario es: ofensivo en alg˙n sentido, irrelevante, trivial, contiene errores de lenguaje, contiene arengas polÝticas, obedece a fines comerciales, contiene datos de alguna persona en particular, o sugiere cambios en el manejo de pacientes que no hayan sido publicados previamente en alguna revista con revisiˇn por pares.
A˙n no hay comentarios en este artÝculo.
Para comentar debe iniciar sesiˇn
Medwave publica las vistas HTML y descargas PDF por artÝculo, junto con otras mÚtricas de redes sociales.
Rep˙blica de Colombia, Ministerio de Salud y Protecciˇn Social. Indicadores bßsicos, 2013: situaciˇn de salud en Colombia. Bogotß DC; 2014:15-80. RamÝrez JF. Promociˇn de la salud y prevenciˇn de la enfermedad en el adulto mayor desde una perspectiva investigativa integradora. Hallazgos. 2013;10(20):109-122. | Link |Conthe P, Mßrquez Contreras E, Aliaga PÚrez A, Barragßn GarcÝa B, Fernßndez de Cano MartÝn MN, Gonzßlez Jurado M, et al. Treatment compliance in chronic illness: Current situation and future perspectives. Rev Clin Esp. 2014 Aug-Sep;214(6):336-44. | CrossRef | PubMed |Congreso de la Sociedad Espa˝ola de FarmacÚuticos de Atenciˇn Primaria (SEFAP). Elementos bßsicos del abordaje de la medicaciˇn en el paciente crˇnico: Informaciˇn al paciente, conciliaciˇn, revisiˇn y adherencia. 2012. [on line]. | Link |Kim Y, Evangelista LS. Relationship between illness perceptions, treatment adherence, and clinical outcomes in patients on maintenance hemodialysis. Nephrol Nurs J. 2010 May-Jun;37(3):271-80. | PubMed |Perreault S, Ellia L, Dragomir A, C˘tÚ R, Blais L, BÚrard A, Lalonde L. Effect of statin adherence on cerebrovascular disease in primary prevention. Am J Med. 2009 Jul;122(7):647-55. | CrossRef | PubMed |Meinema JG, van Dijk N, Beune EJ, Jaarsma DA, van Weert HC, Haafkens JA. Determinants of adherence to treatment in hypertensive patients of African descent and the role of culturally appropriate education. PLoS One. 2015 Aug 12;10(8):e0133560. | CrossRef | PubMed |Hernßndez R, Fernßndez C, Baptista P. MetodologÝa de la investigaciˇn. Quinta ediciˇn. MÚxico D.F: Mc Graw Hill; 2010: 362-389. Patel NK, Wood RC, Espino DV. Cultural Considerations: Pharmacological and Nonpharmacological Means for Improving Blood Pressure Control among Hispanic Patients. Int J Hypertens. 2012;2012:831016. | CrossRef | PubMed |Belza B, Walwick J, Shiu-Thornton S, Schwartz S, Taylor M, LoGerfo J. Older adult perspectives on physical activity and exercise: voices from multiple cultures. Prev Chronic Dis. 2004 Oct;1(4):A09. Epub 2004 Sep 15. | PubMed |Herrera M, Barros C, Fernßndez M. Predictors of Quality of Life in Old Age: A Multivariate Study in Chile. Journal of Population Ageing. 2011; 1(1):121-39. | CrossRef |Rep˙blica de Colombia, Congreso de la Rep˙blica. Ley 1315 ôPor medio de la cual se establecen las condiciones mÝnimas que dignifiquen la estadÝa de los adultos mayores en los centros de protecciˇn, centros de dÝa e instituciones de atenciˇn.ö, 2009. | Link |Zelada M, Mayta P. ┐Estamos preparados para la atenciˇn primaria del adulto mayor? Rev Peru Med Exp Salud P˙blica. 2006; 23(1):6769. | CrossRef |Quijada AR. Adulto mayor y sus cuidados en Atenciˇn Primaria de Salud: una mirada a las representaciones sociales sobre el equipo de cabecera y las acciones del programa del adulto mayor en CESFAM Laraquete. Repositorio Acßdemico de la Universidad de Chile. 2011:8-123. | Link |RodrÝguez F, Lˇpez F. Planificaciˇn sanitaria (II): desde la priorizaciˇn de problemas a la elaboraciˇn de un programa de salud. Semergen. 2004;30(4):180-89. | Link |SecretarÝa de Planeaciˇn de Bogotß. Sistema de identificaciˇn y clasificaciˇn de potenciales beneficiarios para programas sociales (SisbÚn). [on line]. | Link |Dennison-Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014 Feb 5;311(5):507-20. | CrossRef | PubMed |Eckel RH, Jakicic JM, Ard JD, de Jesus JM, Houston Miller N, Hubbard VS, et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014 Jul 1;63(25 Pt B):2960-84. | CrossRef | PubMed |Fongwa MN, Evangelista LS, Hays RD, Martins DS, Elashoff D, Cowan MJ, et al. Adherence treatment factors in hypertensive African American women. Vasc Health Risk Manag. 2008;4(1):157-66. | PubMed |Chotisiri L, Yamarat K, Taneepanichskul S. Exploring knowledge, attitudes, and practices toward older adults with hypertension in primary care. J Multidiscip Healthc. 2016 Oct 26;9:559-564. | CrossRef | PubMed |Beune EJ, Moll van Charante EP, Beem L, Mohrs J, Agyemang CO, Ogedegbe G, et al. Culturally adapted hypertension education (CAHE) to improve blood pressure control and treatment adherence in patients of African origin with uncontrolled hypertension: cluster-randomized trial. PLoS One. 2014 Mar 5;9(3):e90103. | CrossRef | PubMed |Odusola AO, Nelissen H, Hendriks M, Schultsz C, Wit F, Bolarinwa OA, et al. How Group-Based Cardiovascular Health Education Affects Treatment Adherence and Blood Pressure Control among Insured Hypertensive Nigerians: A Pre-Test, Post-Test Study. World Journal of Cardiovascular Diseases. 2015; 5:181-98. | Link |Telner D, Bujas-Bobanovic M, Chan D, Chester B, Marlow B, Meuser J, et al. Game-based versus traditional case-based learning: comparing effectiveness in stroke continuing medical education. Can Fam Physician. 2010 Sep;56(9):e345-51. | PubMed |Lombardo-Earl G, Roman-Ramos R, Zamilpa A, Herrera-Ruiz M, Rosas-Salgado G, Tortoriello J, et al. Extracts and Fractions from Edible Roots of Sechium edule (Jacq.) Sw. with Antihypertensive Activity. Evid Based Complement Alternat Med. 2014;2014:594326. | CrossRef | PubMed |Alamgeer, Iman S, Asif H, Saleem M. Evaluation of antihypertensive potential of Ficus carica fruit. Pharm Biol. 2017 Dec;55(1):1047-1053. | CrossRef | PubMed |Howes F, Warnecke E, Nelson M. Barriers to lifestyle risk factor assessment and management in hypertension: a qualitative study of Australian general practitioners. J Hum Hypertens. 2013 Aug;27(8):474-8.
| CrossRef | PubMed |ConceišŃo LS, Neto MG, do Amaral MA, Martins-Filho PR, Oliveira Carvalho V. Effect of dance therapy on blood pressure and exercise capacity of individuals with hypertension: A systematic review and meta-analysis. Int J Cardiol. 2016 Oct 1;220:553-7. | CrossRef | PubMed |Kaholokula JK, Look M, Mabellos T, Zhang G, de Silva M, Yoshimura S, et al. Cultural Dance Program Improves Hypertension Management for Native Hawaiians and Pacific Islanders: a Pilot Randomized Trial. J Racial Ethn Health Disparities. 2017 Feb;4(1):35-46. | CrossRef | PubMed |Abellßn J, Sainz P, OrtÝn EJ. GuÝa para la prescripciˇn de ejercicio fÝsico en pacientes con riesgo cardiovascular. Segunda ediciˇn. Espa˝a: Editorial Industrias Grßficas Libecrom; 2014:169-77. Stubbe JH, Brouwer W, Delnoij DM. Patients' experiences with quality of hospital care: the Consumer Quality Index Cataract Questionnaire. BMC Ophthalmol. 2007 Sep 19;7:14. | PubMed |Newman S, Hatton-Yeo A. Intergenerational Learning and the Contributions of Older People. Ageing Horizons. 2008; 8:31-9. ID20080269849. | Link |Trogdon JG, Larsen B, Larsen D, Salas W, Snell M. Cost-effectiveness evaluation of a collaborative patient education hypertension intervention in Utah. J Clin Hypertens (Greenwich). 2012 Nov;14(11):760-6. | CrossRef | PubMed |Machado AP, Lima BM, Laureano MG, Silva PH, Tardin GP, Reis PS, et al. Educational strategies for the prevention of diabetes, hypertension, and obesity. Rev Assoc Med Bras (1992). 2016 Nov;62(8):800-808. | CrossRef | PubMed |Peixoto R, Pereira C, Branco L, Costa K, Carre˝o R, Silva RT, et al. Integration and continuity of Care in health care network models for frail older adults. Rev Saude Publica. 2014 Apr;48(2):357-65. | PubMed |Nguyen QT, Anderson SR, Sanders L, Nguyen LD. Managing hypertension in the elderly: a common chronic disease with increasing age. Am Health Drug Benefits. 2012 May;5(3):146-53. | PubMed |Velßsquez V, Lˇpez L, Lˇpez H, Cata˝o N, Mu˝oz E. [The effect of an elderly people caregivers' educational program: a cultural perspective]. Rev Salud Publica (Bogota). 2011 Jun;13(3):458-69. | PubMed |Agudelo E, RÝos ML, Gonzßlez ME, Rivera EY, VÚlez HF. Resultados de la capacitaciˇn a cuidadores de Adultos Mayores en el Departamento de Risaralda 2011 (Colombia). Rev Investigaciones Andinas. 2013;27(15):825-37. | Link |Hasandokht T, Farajzadegan Z, Siadat ZD, Paknahad Z, Rajati F. Lifestyle interventions for hypertension treatment among Iranian women in primary health-care settings: Results of a randomized controlled trial. J Res Med Sci. 2015 Jan;20(1):54-61. | PubMed |Gofin J, Gofin R. [Community-oriented primary care: a public health model in primary care]. Rev Panam Salud Publica. 2007 Feb-Mar;21(2-3):177-84. | PubMed |






 Estudios originales
Estudios originales