
Key Words: dual practice, public policies, Epistemonikos, GRADE
Abstract
INTRODUCTION
Dual practice (i.e. workers who work in the public and private sector) has an impact on health services in terms of quality and costs. However, the effectiveness of regulatory policies has not been proven.
METHODS
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS
We identified three systematic reviews that included 23 primary studies overall, of which all correspond to observational studies. We concluded it is not clear whether the interventions to reduce the negative consequences of dual practice in the health system are effective because the certainty of the available evidence is very low.
Problem
Dual practice is a common phenomenon in mixed health systems with the participation of public and private actors. The definition most frequently used is ‘to carry out more than one job’ [1]. In low- and middle-income countries, it has negative effects on the public sector, leading to a deficit of human resources, low salaries and poor working conditions secondary to the growth of the private sector [1].
Although the impact of these practices depends on the context of each country, the negative effects on the public system seem to prevail. This translates, for example, into conflicts of interest where professionals provide suboptimal care, in terms of quality or timeliness, in order to transfer them to the private system [1]. Likewise, dual practice would cause difficulties for the public sector to retain the necessary human resources to satisfy the demand of the population [2]. Despite the observation of the potential negative effects of dual practice on health systems, there is still controversy about the effectiveness of regulatory alternatives to avoid these consequences.
Methods
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We found three systematic reviews [1], [3], [4] that included 23 primary studies [5], [6], [7], [8], [9], [10], [11], [12], [13], [14], [15], [16], [17], [18], [19], [20], [21], [22], [23], [24], [25], [26], [27], [28] of which, all correspond to observational studies. |
|
What kind of countries were included* |
The 23 studies were carried out in countries from different income levels, analyzing physicians or heterogeneous groups that included all types of health professionals. |
|
What types of interventions were included* |
All the studies evaluated the effect on the public sector of regulatory policies at a national level. |
|
What types of outcomes |
The outcomes, as grouped by the systematic reviews, were the following: migration of professionals to the private sector, quality of care and migration of patients to the private sector. |
* The information about primary studies is extracted from the systematic reviews identified, unless otherwise specified.
Summary of findings
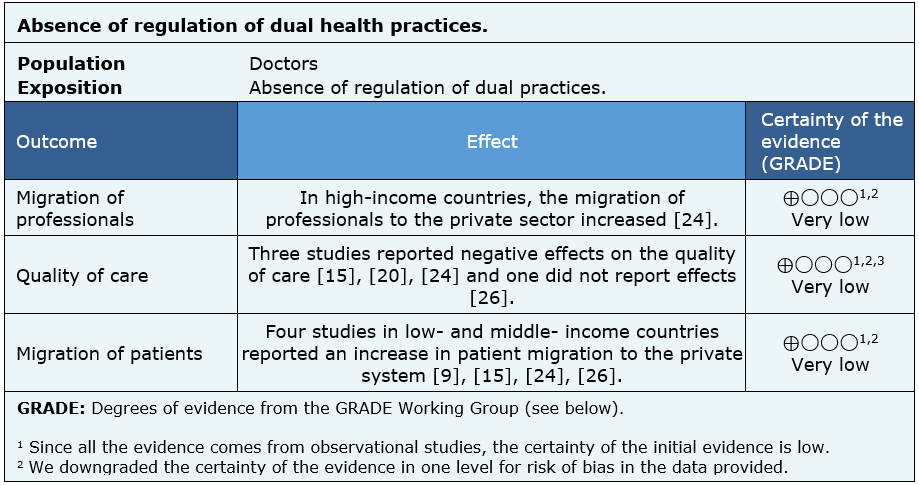
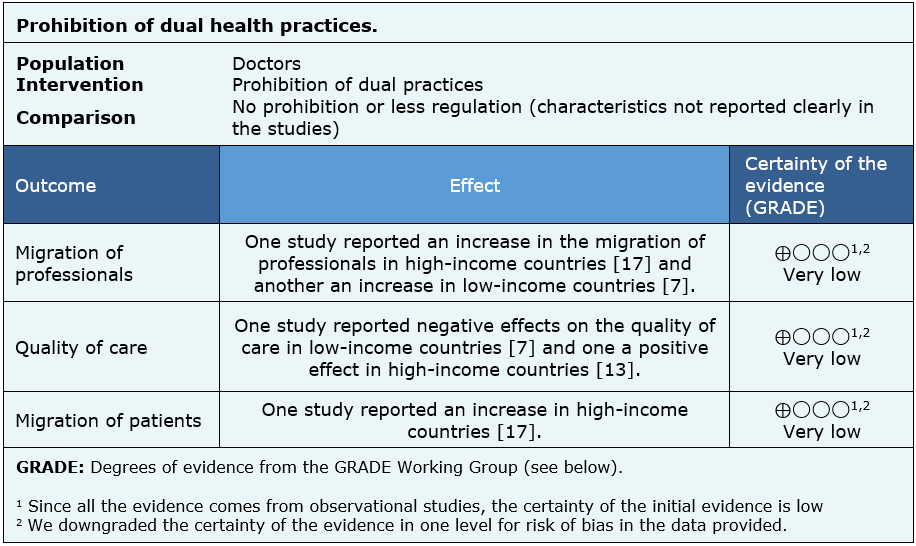
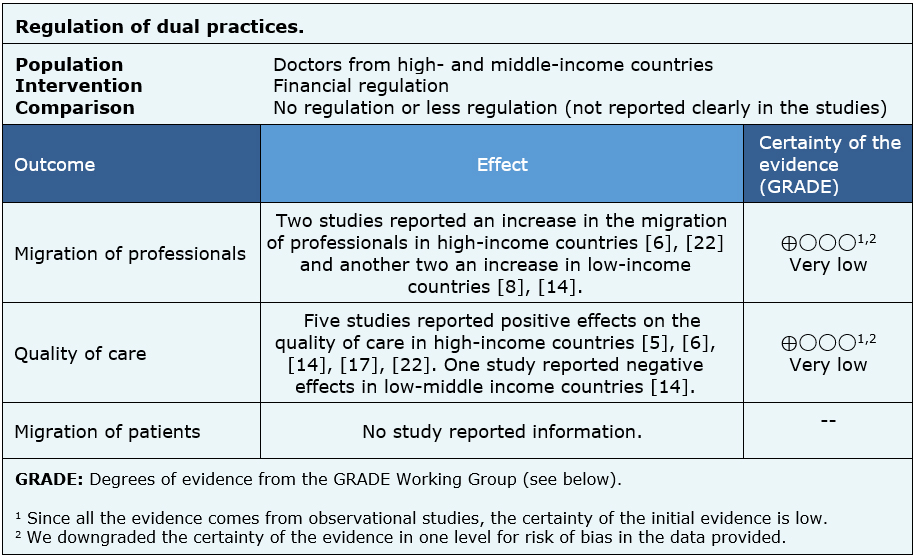
The information on the effects of regulation of dual practices in the public system is based on 21 of the 23 studies identified [5], [6], [7], [8], [9], [10], [11], [12], [13], [14], [15], [17], [18], [20], [21], [22], [23], [24], [25], [26], [27], since two studies did not report any of the outcomes of interest [16], [19]. Twelve studies reported migration of professionals to the private system [6], [7], [8], [9], [10], [11], [12], [13], [22], [24], [17], [14], fourteen reported quality of care [5], [6], [9], [10], [11], [12], [13] [14], [15], [18], [20], [22], [24], [27] and nine migration of patients to the private system [9], [11], [12], [15], [17], [18], [20], [24], [26].
None of the identified reviews managed to extract the data in a way that could be incorporated into a meta-analysis, so the information presented below corresponds to a narrative synthesis of the information obtained from the reviews.
The summary of findings is as follows:
- It is not clear whether interventions to reduce the negative consequences of dual practices in the health system reduces migration of professionals, because the certainty of the available evidence is very low.
- It is not clear whether interventions to reduce the negative consequences of dual practices in the health system improve the quality of care, because the certainty of the available evidence is very low.
- It is not clear whether interventions to reduce the negative consequences of dual practices in the health system reduce patient migration, because the certainty of the available evidence is very low.

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would doctors and countries think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
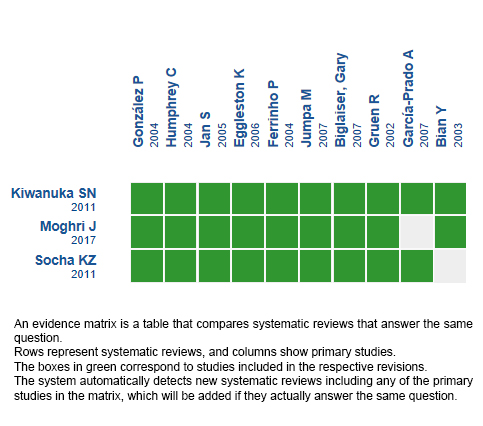
Follow the link to access the interactive version: Regulation of dual practice in the health sector.
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
 Esta obra de Medwave estß bajo una licencia Creative Commons Atribuci¾n-NoComercial 3.0 Unported. Esta licencia permite el uso, distribuci¾n y reproducci¾n del artĒculo en cualquier medio, siempre y cuando se otorgue el crķdito correspondiente al autor del artĒculo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave estß bajo una licencia Creative Commons Atribuci¾n-NoComercial 3.0 Unported. Esta licencia permite el uso, distribuci¾n y reproducci¾n del artĒculo en cualquier medio, siempre y cuando se otorgue el crķdito correspondiente al autor del artĒculo y al medio en que se publica, en este caso, Medwave.

INTRODUCCIėN
La prßctica dual (trabajadores que se desempe±an en el sector p·blico y privado) tiene impacto en los servicios de salud en tķrminos de calidad y costos. Sin embargo, la efectividad de polĒticas de regulaci¾n no ha sido demostrada.
M╔TODOS
Realizamos una b·squeda en Epistemonikos, la mayor base de datos de revisiones sistemßticas en salud, la cual es mantenida mediante el cribado de m·ltiples fuentes de informaci¾n, incluyendo MEDLINE, EMBASE, Cochrane, entre otras. Extrajimos los datos desde las revisiones identificadas, analizamos los datos de los estudios primarios, realizamos un metanßlisis y preparamos una tabla de resumen de los resultados utilizando el mķtodo GRADE.
RESULTADOS Y CONCLUSIONES
Identificamos tres revisiones sistemßticas que en conjunto incluyeron 23 estudios primarios, de los cuales, todos corresponden a estudios observacionales. Concluimos que no estß claro si las intervenciones para reducir las consecuencias negativas de la prßctica dual en el sistema de salud son efectivas porque la certeza de la evidencia disponible es muy baja.
Authors:
Cristißn Gonzßlez[1,2], Crist¾bal Cuadrado[1,2]
Affiliation:
[1] Escuela de Salud P·blica, Universidad de Chile, Santiago, Chile
[2] Proyecto Epistemonikos, Santiago, Chile
E-mail: ccuadrado@uchile.cl
Author address:
[1] Escuela de Salud P·blica Universidad de Chile Avda. Independencia 939 Independencia Santiago Chile
Citation: Gonzßlez C, Cuadrado C. Interventions to reduce the impact of dual practice in the public health sector. Medwave 2019;19(5):e7643 doi: 10.5867/medwave.2019.05.7643
Submission date: 13/12/2018
Acceptance date: 8/4/2019
Publication date: 26/6/2019
Origin: This article is a product of the Evidence Synthesis Project of Epistemonikos Fundation, in collaboration with Medwave for its publication.
Type of review: Non-blinded peer review by members of the methodological team of Epistemonikos Evidence Synthesis Project.
Comments (0)
We are pleased to have your comment on one of our articles. Your comment will be published as soon as it is posted. However, Medwave reserves the right to remove it later if the editors consider your comment to be: offensive in some sense, irrelevant, trivial, contains grammatical mistakes, contains political harangues, appears to be advertising, contains data from a particular person or suggests the need for changes in practice in terms of diagnostic, preventive or therapeutic interventions, if that evidence has not previously been published in a peer-reviewed journal.
No comments on this article.
To comment please log in
Medwave provides HTML and PDF download counts as well as other harvested interaction metrics. There may be a 48-hour delay for most recent metrics to be posted.
- Kiwanuka, SN, Kinengyere, AA, Rutebemberwa, E, Nalwadda, C, Ssengooba, F, Olico-Okui, Pariyo, GW. Dual practice regulatory mechanisms in the health sector: A systematic review of approaches and implementation. London: EPPI-Centre, Social Science Research Unit, Institute of Education, University of London. 2011.
- McPake B,Russo G, Hipgrave D, Hort K, Campbell J. Implications of dual practice for universal health coverage. Bulletin of the World Health Organization 2016;94:142-146. | CrossRef |
- Socha KZ, Bech M. Physician dual practice: a review of literature. Health Policy. 2011 Sep;102(1):1-7. | CrossRef | PubMed |
- Moghri J, Rashidian A, Arab M, Akbari Sari A. Implications of Dual Practice among Health Workers: A Systematic Review. Iran J Public Health. 2017 Feb;46(2):153-164. | PubMed | PMC |
- Gonzßlez P. Should physicians' dual practice be limited? An incentive approach. Health Econ. 2004 Jun;13(6):505-24. | PubMed |
- Humphrey C, Russell J. Motivation and values of hospital consultants in south-east England who work in the national health service and do private practice. Soc Sci Med. 2004 Sep;59(6):1241-50. | PubMed |
- Oliveira MD, Pinto CG. Health care reform in Portugal: an evaluation of the NHS experience. Health Econ. 2005 Sep;14(Suppl 1):S203-20. | PubMed |
- GarcĒa-Prado A, Gonzßlez P. Policy and regulatory responses to dual practice in the health sector. Health Policy. 2007 Dec;84(2-3):142-52. | PubMed |
- Jan S, Bian Y, Jumpa M, Meng Q, Nyazema N, Prakongsai P, Mills A. Dual job holding by public sector health professionals in highly resource-constrained settings: problem or solution? Bull World Health Organ. 2005 Oct;83(10):771-6. | PubMed | PMC |
- Eggleston K, Bir A. Physician dual practice. Health Policy. 2006 Oct;78(2-3):157-66. | PubMed |
- Ferrinho P, Van Lerberghe W, Fronteira I, Hip¾lito F, Biscaia A. Dual practice in the health sector: review of the evidence. Hum Resour Health. 2004 Oct 27;2(1):14. | PubMed | PMC |
- Jumpa M, Jan S, Mills A. The role of regulation in influencing income-generating activities among public sector doctors in Peru. Hum Resour Health. 2007 Feb 26;5:5. | PubMed | PMC |
- Mossialos E, Allin S, Davaki K. Analysing the Greek health system: a tale of fragmentation and inertia. Health Econ. 2005 Sep;14(Suppl 1):S151-68. | PubMed |
- GarcĒa-Prado A, Gonzßlez P. Whom do physicians work for? An analysis of dual practice in the health sector. J Health Polit Policy Law. 2011 Apr;36(2):265-94. | CrossRef | PubMed |
- Gruen R, Anwar R, Begum T, Killingsworth JR, Normand C. Dual job holding practitioners in Bangladesh: an exploration. Soc Sci Med. 2002 Jan;54(2):267-79. | PubMed |
- De Pietro C. Private medical services in the Italian public hospitals: the case for improving HRM. Health Policy. 2006 Aug 22;78(1):56-69. | PubMed |
- Gonzßlez P, Macho-Stadler I. A theoretical approach to dual practice regulations in the health sector. J Health Econ. 2013 Jan;32(1):66-87. | CrossRef | PubMed |
- Biglaiser, Gary, Albert Ma, Ching-to. Moonlighting: public service and private practice. The RAND Journal of Economics. 2007;38(4):1113-1133.
- Sµther, Erik Magnus. A Discrete Choice Analysis of Norwegian PhysiciansÆ Labor Supply and Sector Choice. Oslo University, Health Economics Research Programme. 2009.
- Ensor T, Duran-Moreno A. Corruption as a challenge in effective regulation in the health sector. Regulating entrepreneurial behaviour in European health care systems. Open University Press. 2002;:106-24.
- Bian Y, Sun Q, Jan S, Yu J, Meng Q. Dual practice by public health providers in Shandong and Sichuan Province, China. London: Health Economics and Financing Programme, London School of Hygiene and Tropical Medicine. 2003.
- Prakongsai P, Chindawatana W, Tantivess S, Mugem S, Tangcharoensathien V. Dual practice among public medical doctors in Thailand. Dual practice among public medical doctors in Thailand. 2003.
- Amirault T. Characteristics of multiple jobholders. Monthly Labor Review. 1997;120:9-15.
- Chue Pholeng. Incentives to Dual Practice New Institutional Economic analysis of CanadaÆs mixed public-private health sector. Econ Theses. 2007.
- Akbari Sari A, Babashahy S, Ghanati E, Naderi M, Tabatabaei Lotfi SM, Olyaee Manesh A, et al. Implementing the full-time practice in Iran health system; perceptions of the medical university chancellors on its challenges, consequences and effective solutions. 2013.
- Jiwei Q. (2010). Financing health in China: Theory & institutions. National university of Singapore.
- Berman P, Cuizon D. (2004). Multiple public-private jobholding of health care providers in developing countries. Issues Paper¢Private Sector, London: DFID Health Systems Resource Centre.
Kiwanuka, SN, Kinengyere, AA, Rutebemberwa, E, Nalwadda, C, Ssengooba, F, Olico-Okui, Pariyo, GW. Dual practice regulatory mechanisms in the health sector: A systematic review of approaches and implementation. London: EPPI-Centre, Social Science Research Unit, Institute of Education, University of London. 2011. McPake B,Russo G, Hipgrave D, Hort K, Campbell J. Implications of dual practice for universal health coverage. Bulletin of the World Health Organization 2016;94:142-146. | CrossRef |Socha KZ, Bech M. Physician dual practice: a review of literature. Health Policy. 2011 Sep;102(1):1-7. | CrossRef | PubMed |Moghri J, Rashidian A, Arab M, Akbari Sari A. Implications of Dual Practice among Health Workers: A Systematic Review. Iran J Public Health. 2017 Feb;46(2):153-164. | PubMed | PMC |Gonzßlez P. Should physicians' dual practice be limited? An incentive approach. Health Econ. 2004 Jun;13(6):505-24. | PubMed |Humphrey C, Russell J. Motivation and values of hospital consultants in south-east England who work in the national health service and do private practice. Soc Sci Med. 2004 Sep;59(6):1241-50. | PubMed |Oliveira MD, Pinto CG. Health care reform in Portugal: an evaluation of the NHS experience. Health Econ. 2005 Sep;14(Suppl 1):S203-20. | PubMed |GarcĒa-Prado A, Gonzßlez P. Policy and regulatory responses to dual practice in the health sector. Health Policy. 2007 Dec;84(2-3):142-52. | PubMed |Jan S, Bian Y, Jumpa M, Meng Q, Nyazema N, Prakongsai P, Mills A. Dual job holding by public sector health professionals in highly resource-constrained settings: problem or solution? Bull World Health Organ. 2005 Oct;83(10):771-6. | PubMed | PMC |Ferrinho P, Van Lerberghe W, Fronteira I, Hip¾lito F, Biscaia A. Dual practice in the health sector: review of the evidence. Hum Resour Health. 2004 Oct 27;2(1):14. | PubMed | PMC |Jumpa M, Jan S, Mills A. The role of regulation in influencing income-generating activities among public sector doctors in Peru. Hum Resour Health. 2007 Feb 26;5:5. | PubMed | PMC |Mossialos E, Allin S, Davaki K. Analysing the Greek health system: a tale of fragmentation and inertia. Health Econ. 2005 Sep;14(Suppl 1):S151-68. | PubMed |GarcĒa-Prado A, Gonzßlez P. Whom do physicians work for? An analysis of dual practice in the health sector. J Health Polit Policy Law. 2011 Apr;36(2):265-94. | CrossRef | PubMed |Gruen R, Anwar R, Begum T, Killingsworth JR, Normand C. Dual job holding practitioners in Bangladesh: an exploration. Soc Sci Med. 2002 Jan;54(2):267-79. | PubMed |De Pietro C. Private medical services in the Italian public hospitals: the case for improving HRM. Health Policy. 2006 Aug 22;78(1):56-69. | PubMed |Gonzßlez P, Macho-Stadler I. A theoretical approach to dual practice regulations in the health sector. J Health Econ. 2013 Jan;32(1):66-87. | CrossRef | PubMed |Biglaiser, Gary, Albert Ma, Ching-to. Moonlighting: public service and private practice. The RAND Journal of Economics. 2007;38(4):1113-1133. Sµther, Erik Magnus. A Discrete Choice Analysis of Norwegian PhysiciansÆ Labor Supply and Sector Choice. Oslo University, Health Economics Research Programme. 2009. Ensor T, Duran-Moreno A. Corruption as a challenge in effective regulation in the health sector. Regulating entrepreneurial behaviour in European health care systems. Open University Press. 2002;:106-24. Bian Y, Sun Q, Jan S, Yu J, Meng Q. Dual practice by public health providers in Shandong and Sichuan Province, China. London: Health Economics and Financing Programme, London School of Hygiene and Tropical Medicine. 2003. Prakongsai P, Chindawatana W, Tantivess S, Mugem S, Tangcharoensathien V. Dual practice among public medical doctors in Thailand. Dual practice among public medical doctors in Thailand. 2003. Amirault T. Characteristics of multiple jobholders. Monthly Labor Review. 1997;120:9-15. Chue Pholeng. Incentives to Dual Practice New Institutional Economic analysis of CanadaÆs mixed public-private health sector. Econ Theses. 2007. Akbari Sari A, Babashahy S, Ghanati E, Naderi M, Tabatabaei Lotfi SM, Olyaee Manesh A, et al. Implementing the full-time practice in Iran health system; perceptions of the medical university chancellors on its challenges, consequences and effective solutions. 2013. Jiwei Q. (2010). Financing health in China: Theory & institutions. National university of Singapore. Berman P, Cuizon D. (2004). Multiple public-private jobholding of health care providers in developing countries. Issues Paper¢Private Sector, London: DFID Health Systems Resource Centre. 





 Research papers
Research papersSystematization of initiatives in sexual and reproductive health about good practices criteria in response to the COVID-19 pandemic in primary health care in Chile
Clinical, psychological, social, and family characterization of suicidal behavior in Chilean adolescents: a multiple correspondence analysis
