
Key Words: aorta torácica; tomografía; variantes anatómicas
Abstract
PURPOSE
Previous publications from two countries in South America found one anatomical variation not previously reported in the rest of the world, which in turn give some clues with regard to a racial difference. The objective of the present study is to describe variations in the anatomical distribution of the branches of the aortic arch in a Peruvian population.
OBJECTIVE
To describe variations in the anatomical distribution of the branches of the aortic arch in a Peruvian population
METHODS
A descriptive study of patients who underwent a tomography angiography of the aorta was performed. We analyzed the reports that showed the description of the variations of the branches of the aortic arch based on the eight types currently described in the literature.
RESULTS
From 361 analyzed reports, 282 patients (78.12%) had a normal aortic arch configuration (type I; aortic arch gives rise to the brachiocephalic trunk, left common carotid and left subclavian arteries); followed by type II (left common carotid artery as a branch of the aorta) with 41 patients (11.36%); and type IX (common ostium for the brachiocephalic trunk and the left common carotid artery) with 25 patients (6.93%). The latter and two other types are new variations.
CONCLUSION
Aortic Arch Type I, Type II and Type IX were the most frequent variations in this Peruvian study. Additionally, we also found two more new types that have not been previously described in the literature. Further investigation regarding these variations is needed in order to assess a racial factor in South America and possible relationships with clinical or surgical events.
Introduction
The “normal” configuration of the aortic arch has three branches: A brachiocephalic trunk (BT), which gives rise to the right subclavian (RS) and the right common carotid (RCC), a left common carotid (LCC), and a left subclavian (LS) artery [1]. The variations of the anatomical configuration of the aortic arch are reported from 6 to 49% of the studied population in several countries [1],[2],[3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14]. However, there is no information regarding the frequency of these variations in Latin American population [1],[2],[3],[4],[5],[6],[7],[8].
Two publications from Colombia and Argentina identified a not previously reported variation, which implies a racial difference in this area of South America when compared to the rest of the published articles regarding this matter [15],[16].
The majority of the aortic arch branches variations are described as asymptomatic, although others have been associated with relevant symptomatology and serious surgical problems, secondary to compression or pressure of the trachea or esophagus [17],[18],[19],[20],[21],[22],[23],[24]. If the physician does not take into consideration the existence of those possibilities, the diagnosis dilates and the costs increase. In our country, unpublished articles related to these variations generate a degree of uncertainty in clinical, radiological and, interventionist practice.
For example, an aberrant vertebral artery as a branch of the aorta is an extremely important variation when cervical vascular surgery is performed, since it will give complications [17],[23]. Apart from that, some authors have suggested that the anomalous origin of the vertebral arteries, coupled with a more extensive vascular path, may cause hemodynamic disturbances that predispose to cerebrovascular diseases [10],[15], whereas others argue that the artery would have a greater flow as it receives the blood directly from the heart; and that the large extension of the artery could affect the hemodynamic resistance of the vessels, thus causing fatigue in the distal portion of the artery [10],[23].
The objective of our study was to describe variations in the anatomical distribution of the branches of the aortic arch in a Peruvian population.
Methods
Study Design, Population and inclusion criteria
This is a descriptive study involving analysis of a series of cases in a Peruvian population. 361 reports of Multislice CT Spiral Angiography (MSCTA), performed by two experienced radiologists of the imaging center “RESOMASA”, during the period 2004-2009, were reviewed. All the MSCTA reports that described the anatomic distribution of the branches of the aortic arch were included in the study, excluding the reports that could have contradictory or incomplete information. Aside from the origin of the population and the sex of the individual, no other sociodemographic variables were included in the study due to the lack of effect of those variables into the embryologic and anatomic configuration of the aortic arch [4].
Procedures for collecting information
The electronic reports were collected in RESOMASA, assigning a code to each one, and then copied to a Compact Disc - Read-Only Memory (CD-ROM) and kept by the researchers for subsequent discharge in the database.
Center and equipment
RESOMASA is a specialized reference center for imaging diagnosis by magnetic resonance and multislice spiral computer tomography SOMATON SENSATION CARDIAC (Siemens Medical Systems, Erlangen, Germany), is located in the department of Lima, the Peruvian capital. RESOMASA is medical team of specialists recognized for their experience and expertise, as well as the accuracy of their images. Since it is a private center, people pay for the imaging tests. The MSCTA report is filled using a format where all the arteries must be specified, thus avoiding an observer omission.
Classification of types of aortic arches
We used the rating by Natsis et al. in his revision article published in 2009 [3]. See table 1.
The other types of aortic arch found continued this classification, being referred to as Type IX, X and XI. See table 2.
Table 1. Types of aortic arches according to Natsis, et al.
Table 2 New types of Aortic Arch.
Statistical analysis
The analysis was performed with STATA statistical software version 10, elaborating frequency tables for the analysis of the qualitative variables.
Ethical issues
The study protocol followed the standards norms of the Helsinki declaration and was approved by the Institutional Ethics Committee of the “Universidad Peruana Cayetano Heredia” and RESOMASA authorities. No names or addresses of the patients were included in the study. The authors signed a letter of commitment to confidentiality of the data.
Results
361 reports were included according to our criteria. We found 7 different distributions of the branches of the aortic arch, reporting 3 new types in this population. See table 2. The type I or classic was the most frequent with 275 cases (78.12%), followed by the type II with 41 cases (11.36%), type IX with 25 cases (6.93%), type III with 8 cases (2.22%), type V with 3 cases (0.83%) and type X and XI with 1 case each one. The three new types frequency as well as the frequency of all the other types found are described in table 3. Type IV, VI, VII or VIII variations were not found in our population. The images of the configuration of each aortic arch are shown in Figs. 1 and 2.
Table 3. Type of aortic arch frequency.
Figure 1. Diagram of types of aortic arches according to Natsis et al.
Discussion
We used the classification of Natsis et al. [3], who made a scientific review of the majority of the published articles on anatomical variations of the aortic arch, categorizing them according to their incidences. In our study, angiography was employed by MSCTA, technique that has shown an excellent correlation with conventional angiography, even in coronary artery atherosclerotic disease [25],[26],[27].
Type I was the most frequent aortic arch configuration reported in our study, which is compatible with other studies worldwide (64.9 - 94.3%) [4],[5],[11]. The second one was type II, whose incidence is also within the range reported in the literature (11-27%) [1],[3],[4]. However, there are two reports with a lover incidence in American-Japanese men (1.03%) [5] and in Polish population (0.9%) [6]. This variation has been rarely associated with clinical symptoms, which were attributed to an expansion of the superior mediastinum [28].
Type III had an incidence of 2.22%. For most authors, this would be the third in terms of incidence (2.5 - 8%) and second to Nelson and Sparks (3.1%) [5]. However, Natsis et al. and Nizankowski et al. reported low frequencies (0.79% and 1.3% respectively) [3],[6]. This variation is very important in neurosurgical and neurovascular interventions because an injury of the vertebral artery is a complication during surgery of the anterior cervical spine, which can cause exsanguination and thus provoke permanent neurological deficits [23]. Furthermore, the vertebral artery can be wrongly considered occluded or diseased when not found by conventional angiography [13]. This variation has only been correlated with clinical symptoms when associated with an intracranial aneurysm [7],[17],[18].
The results of type V are within the described range (0.13% - 25%) with an incidence of 0.83%. Its importance lies in being considered as the cause of "dysphagia lusoria", condition that, despite being asymptomatic in the majority of the cases, could provoke difficult in swallowing and, in some cases, pain due to the pressure exerted by the aberrant artery over the wall of the esophagus, which in turn may need surgical management [29]. It has also been described to cause shortness of breath when the right subclavian meets the trachea. Complications may arise during the tracheostomy if it was found in front of the trachea [30].
We described a variation of the aortic arch that has only been reported in two small series of cases in south-American countries (Colombia and Argentina) [15],[16]. In one article, the authors merely described it as an isolated finding in the part of results [16], whereas the second tried to establish a possible relationship between some variations and the distribution plates of atheroma [15], neither of them highlighting the finding. We called it variation IX, continuing with Natsis classification. Of note, it was the third most common in our series of cases (6.93%) and it is not among the 8 most frequent variations in the literature. Unlike type II, this variation has a common ostium for BT and the LCC. We think that it would be very important to conduct further studies to find out if a relationship with clinical or surgical events exists, as the hemodynamics in a common ostium should be different.
Two more variations of the aortic arch were also found, which have not been reported within the eight most common types described in the literature. Nonetheless, their incidence was less than 1% of the population studied. The main limitations of this study is that it is a series of cases and thus the found frequencies cannot be extrapolated to the rest of the Peruvian population, also, since the MSCTA were performed in a private center, patients pay for their imaging study, which means that most of the patients are middle-class or upper-class Peruvians, so there might be a higher prevalence of some variations in the poorest regions in Peru that are underestimated. However, we believe that an epidemiological study of different populations of our country and from other countries should be performed.
We conclude that in our Peruvian series of cases, the distribution of the branches of the aortic arch of types I, II and IX were the most frequent, the latter being a possible genuine type in south-Americans. In addition, two new not previously described variations were reported. Further investigation regarding this variations is needed in order to assess a racial factor in south-America and possible relationships with clinical or surgical events.
Notes
From the editor
This article was originally submitted in Spanish and was translated into English by the authors. The Journal has not copyedited this version.
Acknowledgments
The authors are grateful to Dr. Pedro Tapia Puente-Arnao and the institution RESOMASA for their selfless support to research, provide all facilities and assistance relating to access its database.
Conflicts of interests
The authors have completed the ICMJE Conflict of Interest form and have no relevant interests to declare.

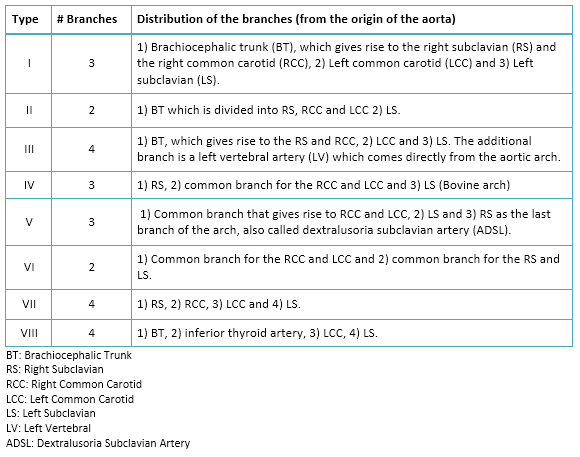 Table 1. Types of aortic arches according to Natsis, et al.
Table 1. Types of aortic arches according to Natsis, et al.
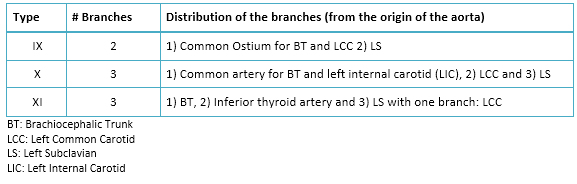 Table 2 New types of Aortic Arch.
Table 2 New types of Aortic Arch.
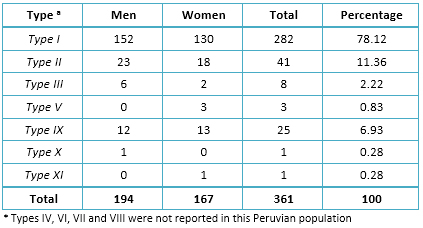 Table 3. Type of aortic arch frequency.
Table 3. Type of aortic arch frequency.
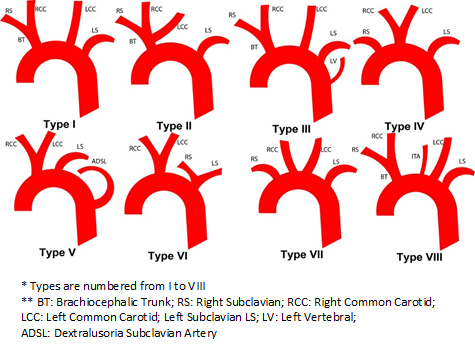 Figure 1. Diagram of types of aortic arches according to Natsis et al.
Figure 1. Diagram of types of aortic arches according to Natsis et al.
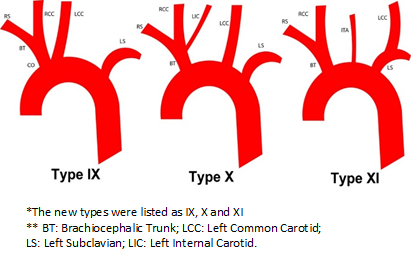 Figure 2. Diagram of the new types of aortic arches found. The new types were listed as IX, X and XI.
Figure 2. Diagram of the new types of aortic arches found. The new types were listed as IX, X and XI.
 Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
INTRODUCCIÓN
Reportes previos en dos países de América del Sur encontraron una variante anatómica que no había sido reportada en el resto del mundo, lo que podría dar indicios acerca de una diferencia racial.
OBJETIVO
Describir las variaciones en la distribución anatómica de las ramas del arco aórtico en una población peruana.
MÉTODOS
Estudio retrospectivo de una serie de casos de personas en quienes se realizó una angiografía por tomografía de la aorta torácica. Se analizaron los informes que registraron la descripción de las variaciones de las ramas del arco aórtico, basados en los ocho tipos descritos por la literatura científica.
RESULTADOS
Se analizaron 361 informes. Se encontró que 282 pacientes (78,12%) tuvieron la configuración clásica (tipo I, arco aórtico que da origen al tronco braquiocefálico, a la carótida común izquierda y a la subclavia izquierda), seguido por el tipo II (arteria carótida común izquierda como rama del tronco braquiocefálico) con 41 pacientes (11,36%), y el tipo IX (un ostium común para el tronco braquiocefálico y la carótida común izquierda) con 25 pacientes (6,93%). Este último y otros dos tipos resultaron ser nuevas variantes del arco aórtico.
CONCLUSIÓN
En esta serie de casos peruana, los tipos de arco aórtico I, II y IX fueron los más frecuentes. Adicionalmente, se encontraron otros dos tipos nuevos que no habían sido descritos en la literatura previamente. Es necesario profundizar la investigación sobre estas variantes para evaluar el factor racial en Sudamérica y una posible relación con eventos clínicos o quirúrgicos.
Authors:
Julio Arturo Huapaya[1], Kristhy Chávez-Trujillo[1], Miguel Trelles[2], Roy Dueńas Carbajal[3], Renato Ferrandiz Espadin[1]
E-mail: julioarturo30@gmail.com
Citation: Huapaya JA, Chávez-Trujillo K, Trelles M, Dueńas Carbajal R, Ferrandiz Espadin R. Anatomic variations of the branches of the aortic arch in a Peruvian population. Medwave 2015 Jul;15(6):e6194 doi: 10.5867/medwave.2015.06.6194
Submission date: 9/5/2015
Acceptance date: 21/7/2015
Publication date: 31/7/2015
Type of review: reviewed by three external peer reviewers, double-blind
Comments (0)
We are pleased to have your comment on one of our articles. Your comment will be published as soon as it is posted. However, Medwave reserves the right to remove it later if the editors consider your comment to be: offensive in some sense, irrelevant, trivial, contains grammatical mistakes, contains political harangues, appears to be advertising, contains data from a particular person or suggests the need for changes in practice in terms of diagnostic, preventive or therapeutic interventions, if that evidence has not previously been published in a peer-reviewed journal.
No comments on this article.
To comment please log in
Medwave provides HTML and PDF download counts as well as other harvested interaction metrics. There may be a 48-hour delay for most recent metrics to be posted.
- Liechty JD, Shields TW, Anson BJ. Variations pertaining to the aortic arches and their branches; with comments on surgically important types. Q Bull Northwest Univ Med Sch. 1957;31(2):136-43. | PubMed |
- McDonald JJ, Anson BJ (1940) Variations in the origin of arteries derived from the aortic arch, in American whites and negroes. American Journal of Physical Anthropology. 1940;27(1):91-107.
- Natsis KI, Tsitouridis IA, Didagelos MV, Fillipidis AA, Vlasis KG, Tsikaras PD. Anatomical variations in the branches of the human aortic arch in 633 angiographies: clinical significance and literature review. Surg Radiol Anat. 2009 Jun;31(5):319-23. | CrossRef | PubMed |
- Nayak SR, Pai MM, Prabhu LV, D'Costa S, Shetty P. Anatomical organization of aortic arch variations in the India: embryological basis and review. Jornal Vascular Brasileiro. 2006;5(2):95-100.
- Bhatia K, Ghabriel MN, Henneberg M. Anatomical variations in the branches of the human aortic arch: a recent study of a South Australian population. Folia Morphol (Warsz). 2005 Aug;64(3):217-23. | PubMed |
- Grande NR, Costa e Silva A, Pereira AS, Aguas AP. Variations in the anatomical organization of the human aortic arch. A study in a Portuguese population. Bull Assoc Anat (Nancy). 1995 Mar;79(244):19-22. | PubMed |
- Shin IY, Chung YG, Shin WH, Im SB, Hwang SC, Kim BT. A morphometric study on cadaveric aortic arch and its major branches in 25 korean adults : the perspective of endovascular surgery. J Korean Neurosurg Soc. 2008 Aug;44(2):78-83. | CrossRef | PubMed |
- Weber TF, Ganten MK, Böckler D, Geisbüsch P, Kopp-Schneider A, Kauczor HU, et al. Assessment of thoracic aortic conformational changes by four-dimensional computed tomography angiography in patients with chronic aortic dissection type b. Eur Radiol. 2009 Jan;19(1):245-53. | CrossRef | PubMed |
- Nelson ML, Sparks CD. Unusual aortic arch variation: distal origin of common carotid arteries. Clin Anat. 2001;14(1):62-5. | PubMed |
- Nizankowski C, Rajchel Z, Ziólkowski M. Abnormal origin of arteries from the aortic arch in man. Folia Morphol (Warsz). 1975;34(2):109-16. | PubMed |
- Albayram S, Gailloud P, Wasserman BA. Bilateral arch origin of the vertebral arteries. AJNR Am J Neuroradiol. 2002 Mar;23(3):455-8. | PubMed |
- Gielecki JS, Wilk R, Syc B, Musiał-Kopiejka M, Piwowarczyk-Nowak A. Digital-image analysis of the aortic arch's development and its variations. Folia Morphol (Warsz). 2004 Nov;63(4):449-54. | PubMed |
- Goray VB, Joshi AR, Garg A, Merchant S, Yadav B, Maheshwari P. Aortic arch variation: a unique case with anomalous origin of both vertebral arteries as additional branches of the aortic arch distal to left subclavian artery. AJNR Am J Neuroradiol. 2005 Jan;26(1):93-5. | PubMed |
- Gupta M, Sodhi L. Variations in branching pattern, shape, size and relative distances of arteries arising from arch of aorta. Nepal Med Coll J. 2005 Jun;7(1):13-7. | PubMed |
- Yeri LA, Gómez JE, Fontaneto S, Espósito M. Variation of the Origin of Aortic Arch Branches: In Relationship with Plates of Atheroma. International Journal of Morphology. 2001;29(1):182-186. | Link |
- Rojas JD, Ballesteros LE. Ramas Emergentes del Arco Aórtico en Fetos Humanos. Un Estudio Descriptivo Directo en Población Colombiana. Int J Morphol. 2009;27(4):989-996.
- Komiyama M, Morikawa T, Nakajima H, Nishikawa M, Yasui T. High incidence of arterial dissection associated with left vertebral artery of aortic origin. Neurol Med Chir (Tokyo). 2001 Jan;41(1):8-11; discussion 11-2. | PubMed |
- Sora MC, Strobl B, Förster-Streffleur S, Staykov D. Aortic arch variation analyzed by using plastination. Clin Anat. 2002 Nov;15(6):379-82. | PubMed |
- Weinberg PM. Aortic arch anomalies. J Cardiovasc Magn Reson. 2006;8(4):633-43. | PubMed |
- Daniel Algieri R, Mazzoglio y Nabar MJ, Ferrante MS. Variación Retroesofágica del Arco Aórtico. International Journal of Morphology. 2008;26(2):337-43. | CrossRef |
- Lu J, Ebraheim NA. The vertebral artery: surgical anatomy. Orthopedics. 1999 Nov;22(11):1081-5. | PubMed |
- Lemke AJ, Benndorf G, Liebig T, Felix R. Anomalous origin of the right vertebral artery: review of the literature and case report of right vertebral artery origin distal to the left subclavian artery. AJNR Am J Neuroradiol. 1999 Aug;20(7):1318-21. | PubMed |
- Hu N, Christensen DA, Agrawal AK, Beaumont C, Clark EB, Hawkins JA. Dependence of aortic arch morphogenesis on intracardiac blood flow in the left atrial ligated chick embryo. Anat Rec (Hoboken). 2009 May;292(5):652-60. | CrossRef | PubMed |
- Juraszek AL, Guleserian KJ. Common aortic arch anomalies: diagnosis and management. Curr Treat Options Cardiovasc Med. 2006 Sep;8(5):414-8. | PubMed |
- Hoffmann MH, Shi H, Schmitz BL, Schmid FT, Lieberknecht M, Schulze R, et al. Noninvasive coronary angiography with multislice computed tomography. JAMA. 2005 May 25;293(20):2471-8. Erratum in: JAMA. 2005 Sep 14;294(10):1208. | PubMed |
- Hollander JE, Chang AM, Shofer FS, McCusker CM, Baxt WG, Litt HI. Coronary computed tomographic angiography for rapid discharge of low-risk patients with potential acute coronary syndromes. Ann Emerg Med. 2009 Mar;53(3):295-304. | CrossRef | PubMed |
- Schuijf JD, Bax JJ, Salm LP, Jukema JW, Lamb HJ, van der Wall EE, de Roos A. Noninvasive coronary imaging and assessment of left ventricular function using 16-slice computed tomography. Am J Cardiol. 2005 Mar 1;95(5):571-4. | PubMed |
- Karkoulias KP, Efremidis GK, Tsiamita MS, Trakada GP, Prodromakis EN, Nousi ED, et al. Abnormal origin of the left common carotid artery by innominate artery: a case of enlargement mediastinum. Monaldi Arch Chest Dis. 2003 Jul-Sep;59(3):222-3. | PubMed |
- Backer CL, Ilbawi MN, Idriss FS, DeLeon SY. Vascular anomalies causing tracheoesophageal compression. Review of experience in children. J Thorac Cardiovasc Surg. 1989 May;97(5):725-31. | PubMed |
- Chadha NK, Chiti-Batelli S. Tracheostomy reveals a rare aberrant right subclavian artery; a case report. BMC Ear Nose Throat Disord. 2004 Mar 30;4(1):1. | PubMed |
- Chadha NK, Chiti-Batelli S. Tracheostomy reveals a rare aberrant right subclavian artery; a case report. BMC Ear Nose Throat Disord. 2004 Mar 30;4(1):1. | PubMed |
Liechty JD, Shields TW, Anson BJ. Variations pertaining to the aortic arches and their branches; with comments on surgically important types. Q Bull Northwest Univ Med Sch. 1957;31(2):136-43. | PubMed |McDonald JJ, Anson BJ (1940) Variations in the origin of arteries derived from the aortic arch, in American whites and negroes. American Journal of Physical Anthropology. 1940;27(1):91-107. Natsis KI, Tsitouridis IA, Didagelos MV, Fillipidis AA, Vlasis KG, Tsikaras PD. Anatomical variations in the branches of the human aortic arch in 633 angiographies: clinical significance and literature review. Surg Radiol Anat. 2009 Jun;31(5):319-23. | CrossRef | PubMed |Nayak SR, Pai MM, Prabhu LV, D'Costa S, Shetty P. Anatomical organization of aortic arch variations in the India: embryological basis and review. Jornal Vascular Brasileiro. 2006;5(2):95-100. Bhatia K, Ghabriel MN, Henneberg M. Anatomical variations in the branches of the human aortic arch: a recent study of a South Australian population. Folia Morphol (Warsz). 2005 Aug;64(3):217-23. | PubMed |Grande NR, Costa e Silva A, Pereira AS, Aguas AP. Variations in the anatomical organization of the human aortic arch. A study in a Portuguese population. Bull Assoc Anat (Nancy). 1995 Mar;79(244):19-22. | PubMed |Shin IY, Chung YG, Shin WH, Im SB, Hwang SC, Kim BT. A morphometric study on cadaveric aortic arch and its major branches in 25 korean adults : the perspective of endovascular surgery. J Korean Neurosurg Soc. 2008 Aug;44(2):78-83. | CrossRef | PubMed |Weber TF, Ganten MK, Böckler D, Geisbüsch P, Kopp-Schneider A, Kauczor HU, et al. Assessment of thoracic aortic conformational changes by four-dimensional computed tomography angiography in patients with chronic aortic dissection type b. Eur Radiol. 2009 Jan;19(1):245-53. | CrossRef | PubMed |Nelson ML, Sparks CD. Unusual aortic arch variation: distal origin of common carotid arteries. Clin Anat. 2001;14(1):62-5. | PubMed |Nizankowski C, Rajchel Z, Ziólkowski M. Abnormal origin of arteries from the aortic arch in man. Folia Morphol (Warsz). 1975;34(2):109-16. | PubMed |Albayram S, Gailloud P, Wasserman BA. Bilateral arch origin of the vertebral arteries. AJNR Am J Neuroradiol. 2002 Mar;23(3):455-8. | PubMed |Gielecki JS, Wilk R, Syc B, Musiał-Kopiejka M, Piwowarczyk-Nowak A. Digital-image analysis of the aortic arch's development and its variations. Folia Morphol (Warsz). 2004 Nov;63(4):449-54. | PubMed |Goray VB, Joshi AR, Garg A, Merchant S, Yadav B, Maheshwari P. Aortic arch variation: a unique case with anomalous origin of both vertebral arteries as additional branches of the aortic arch distal to left subclavian artery. AJNR Am J Neuroradiol. 2005 Jan;26(1):93-5. | PubMed |Gupta M, Sodhi L. Variations in branching pattern, shape, size and relative distances of arteries arising from arch of aorta. Nepal Med Coll J. 2005 Jun;7(1):13-7. | PubMed |Yeri LA, Gómez JE, Fontaneto S, Espósito M. Variation of the Origin of Aortic Arch Branches: In Relationship with Plates of Atheroma. International Journal of Morphology. 2001;29(1):182-186. | Link |Rojas JD, Ballesteros LE. Ramas Emergentes del Arco Aórtico en Fetos Humanos. Un Estudio Descriptivo Directo en Población Colombiana. Int J Morphol. 2009;27(4):989-996. Komiyama M, Morikawa T, Nakajima H, Nishikawa M, Yasui T. High incidence of arterial dissection associated with left vertebral artery of aortic origin. Neurol Med Chir (Tokyo). 2001 Jan;41(1):8-11; discussion 11-2. | PubMed |Sora MC, Strobl B, Förster-Streffleur S, Staykov D. Aortic arch variation analyzed by using plastination. Clin Anat. 2002 Nov;15(6):379-82. | PubMed |Daniel Algieri R, Mazzoglio y Nabar MJ, Ferrante MS. Variación Retroesofágica del Arco Aórtico. International Journal of Morphology. 2008;26(2):337-43. | CrossRef |Lu J, Ebraheim NA. The vertebral artery: surgical anatomy. Orthopedics. 1999 Nov;22(11):1081-5. | PubMed |Lemke AJ, Benndorf G, Liebig T, Felix R. Anomalous origin of the right vertebral artery: review of the literature and case report of right vertebral artery origin distal to the left subclavian artery. AJNR Am J Neuroradiol. 1999 Aug;20(7):1318-21. | PubMed |Hu N, Christensen DA, Agrawal AK, Beaumont C, Clark EB, Hawkins JA. Dependence of aortic arch morphogenesis on intracardiac blood flow in the left atrial ligated chick embryo. Anat Rec (Hoboken). 2009 May;292(5):652-60. | CrossRef | PubMed |Juraszek AL, Guleserian KJ. Common aortic arch anomalies: diagnosis and management. Curr Treat Options Cardiovasc Med. 2006 Sep;8(5):414-8. | PubMed |Hoffmann MH, Shi H, Schmitz BL, Schmid FT, Lieberknecht M, Schulze R, et al. Noninvasive coronary angiography with multislice computed tomography. JAMA. 2005 May 25;293(20):2471-8. Erratum in: JAMA. 2005 Sep 14;294(10):1208. | PubMed |Hollander JE, Chang AM, Shofer FS, McCusker CM, Baxt WG, Litt HI. Coronary computed tomographic angiography for rapid discharge of low-risk patients with potential acute coronary syndromes. Ann Emerg Med. 2009 Mar;53(3):295-304. | CrossRef | PubMed |Schuijf JD, Bax JJ, Salm LP, Jukema JW, Lamb HJ, van der Wall EE, de Roos A. Noninvasive coronary imaging and assessment of left ventricular function using 16-slice computed tomography. Am J Cardiol. 2005 Mar 1;95(5):571-4. | PubMed |Karkoulias KP, Efremidis GK, Tsiamita MS, Trakada GP, Prodromakis EN, Nousi ED, et al. Abnormal origin of the left common carotid artery by innominate artery: a case of enlargement mediastinum. Monaldi Arch Chest Dis. 2003 Jul-Sep;59(3):222-3.
| PubMed |Backer CL, Ilbawi MN, Idriss FS, DeLeon SY. Vascular anomalies causing tracheoesophageal compression. Review of experience in children. J Thorac Cardiovasc Surg. 1989 May;97(5):725-31. | PubMed |Chadha NK, Chiti-Batelli S. Tracheostomy reveals a rare aberrant right subclavian artery; a case report. BMC Ear Nose Throat Disord. 2004 Mar 30;4(1):1. | PubMed |Chadha NK, Chiti-Batelli S. Tracheostomy reveals a rare aberrant right subclavian artery; a case report. BMC Ear Nose Throat Disord. 2004 Mar 30;4(1):1. | PubMed |





 Research papers
Research papersSystematization of initiatives in sexual and reproductive health about good practices criteria in response to the COVID-19 pandemic in primary health care in Chile
Clinical, psychological, social, and family characterization of suicidal behavior in Chilean adolescents: a multiple correspondence analysis
