
Key Words: COVID-19, SARS-CoV-2, otolaryngology, medical education, residency education, skills training
Abstract
Introduction
Coronavirus disease 2019, or COVID-19, has become a global pandemic. Given that the highest viral load of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is found in the airway, otolaryngologists are at high risk of infection. As a result, multiple recommendations have emerged regarding protective measures for surgical teams, including suspending non-urgent procedures and surgeries.
Objectives
To evaluate the impact of the COVID-19 pandemic on otolaryngology residency training programs nationwide.
Methods
A cross-sectional survey-based study was completed in April 2020. The participants were recruited through an online survey, sent by email to all Chilean otolaryngology residents. Demographics, clinical activities, on-call shifts, COVID-19 infection status, exposure to COVID-19 patients, deployment to other specialties, diagnostic/therapeutic procedures, and surgeries performed were analyzed. Self-reported surgical data logs from previous years were used to compare results.
Results
Forty-seven residents completed the survey (84% response rate); 64% of residents refer seeing patients ten days or less during April 2020. Commonly performed procedures such as flexible nasolaryngoscopy, rigid nasal endoscopy, and peritonsillar abscess drainage were not performed by over 40% of the residents in that month. Only 38% participated in surgeries, with an average of 0.6 surgeries as a first surgeon, a dramatic decrease in surgical exposure when comparing the data logs from previous years. Most residents refer the following measures taken by their residency program to improve residency training: bibliographic videoconferences (87%), online clinical case seminars (60%), weekly journal clubs (38%), among others.
Conclusions
Clinical and surgical opportunities decreased dramatically during April 2020. Adjustments to the regular academic curricula should be considered to decrease the negative impact of this pandemic on residency training.
Main messages
|
Introduction
On March 11, 2020, the World Health Organization declared the coronavirus disease (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), as a global pandemic[1]. Given the high airborne viral load[2], otolaryngologists are at a high risk of infection as multiple procedures involve the airway, such as rigid nasal endoscopy, flexible nasolaryngoscopy, anterior nasal packing, tracheostomy, among others. These procedures can also cause aerosolization[3],[4].
As a result, guidelines have been created regarding the protective measures for performing these procedures, including suspending elective procedures and surgeries, minimizing on-call personnel, establishing resident rotation cohorts, and having the most experienced surgeon perform the procedure in the shortest time possible[5],[6],[7],[8].
Taking the above into consideration, and the fact that most otolaryngology outpatient clinics, procedures, and surgeries are optional, we suspected that the COVID-19 pandemic would negatively impact residency training due to the significantly reduced clinical and surgical opportunities[9].
To the best of our knowledge, as of this study’s date, no articles describe the effect of the COVID-19 pandemic on residents’ educational opportunities in Chile.
This study aims to explore the impact of COVID-19 on the otolaryngology residency training programs nationwide and describe the decrease in surgical exposure.
Methods
Clinical opportunity survey
We performed a cross-sectional survey-based study evaluating April 1 to April 30, 2020. There are currently five otolaryngology programs in Chile. Subjects were recruited through a 16-question Google form sent by email to all Chilean otolaryngology residents; the program directors provided contact information.
We obtained demographic data, post-graduate year, and the following information for April 2020: clinical activities, on-call shifts, COVID-19 infection status, exposure to COVID-19 patients, deployment to other specialties, diagnostic/therapeutic procedures performed, and surgeries (first and second surgeons only). We defined COVID-19 positive patients as confirmed by a reverse transcription-polymerase chain reaction and suspected cases when results were pending. Survey response was open from May 11 to May 18, 2020.
Clinical data logs
Historical data logs for specialty diagnostic and therapeutic procedures were only available from student self-reported data logs provided by one residency program from 2017 to 2019: Pontificia Universidad Católica de Chile. Meanwhile, surgeries performed by residents from years prior were only available from student self-reported data logs provided by two residency programs: Pontificia Universidad Católica de Chile and Universidad de Chile, with data from 2017 to 2019 and 2006 to 2016, respectively. Both data logs consisted of procedures or surgeries registered by the residents after their execution. No determination of sample size was required, given the nature of the study.
Data analysis and statistics
This study was approved by the Pontificia Universidad Católica de Chile Ethics Committee (protocol number: 200501001) on May 9, 2020. Electronic informed consent was obtained from all participants before data collection. The data collection was carried out anonymously in an encrypted database. When presenting normal distribution, the descriptive statistics will be expressed with mean and standard deviation. Otherwise, the median was used. The chi-squared test was performed for categorical variables. The means obtained were compared using the student’s T-test. Any P value < 0.05 (significance of 5%) was considered significant.
Results
Forty-seven residents answered the survey, corresponding to an 84% response rate and a mean age of 29.7 ± 3.2 years (range 25-35). Demographic details are shown in Table 1. Six percent of residents were placed initially in preventive quarantine as they belonged to a high-risk group for SARS-CoV-2 infection; 50% (n = 23) provided medical care to a confirmed or suspected COVID-19 patient during April 2020; of them, only 13% (n = 6) needed to undergo preventive quarantine; and one resident tested positive. The average suspected/confirmed patients evaluated per resident was 8.1 ± 8.7 (range 1-30 patients). Thirteen percent (n = 6) of the residents were deployed to a different department as needed by the health care center, with internal medicine being the most frequent (n = 5/6).
Table 1. Demographic data of otolaryngology head and neck surgery residents (n = 47).
Clinical activity
Clinical activities during April 2020 are summarized in Table 2; 65% of the residents spent less than ten days of the month at their corresponding medical health care center, and 68% examined less than eleven patients in outpatient clinics.
Regarding commonly performed procedures, only 55% of the residents performed flexible nasolaryngoscopy, 34% rigid nasal endoscopy, and 21% peritonsillar abscess drainage as seen in Table 3. When analyzing the data obtained from the Pontificia Universidad Católica de Chile residency program, there was a significant decrease in the average procedure per resident for flexible nasolaryngoscopy (13.1 ± 7.5 vs 1.4 ± 1.5, P = 0.001), rigid nasal endoscopy (3.6 ± 2.9 vs 0.4 ± 0.7, P = 0.001), anterior nasal cauterization (0.8 ± 0.5 vs 0.1 ± 0.3, P = 0.002), and fiberoptic endoscopic evaluation of swallowing (3.6 ± 2 vs 0 ± 0, P = 0.000).
Table 3. Quantity of procedures and surgeries performed by the residents during April 2020.
Surgical activity
Of the residents surveyed, 62% (n = 29) did not participate in surgery; of the 18 that did participate, 67% (n = 12) performed as first surgeon, with an average of 0.6 ± 1.2 (range 0-5) surgeries per resident. The most commonly performed surgery was open tracheostomy (n = 6) followed by ethmoidectomy (n = 4), as seen in Table 3. As shown in Figure 1, we observed a dramatic decrease in surgical exposure when comparing data obtained from the Pontificia Universidad Católica de Chile and the Universidad de Chile.
Figure 1. Comparison of Surgeries Performed by Residents.
Educational tools
Residents were asked to provide information relating to measures taken by their residency program in order to promote continuing education and distance learning. Most residents reference bibliographic videoconferences (87%, n = 41), and online clinical case seminars (60%, n = 28). Other measures included weekly journal clubs (38%, n = 18), bibliographical reviews (34%, n = 16), online surgical skills video analysis (15%, n = 7), simulation opportunities (17%, n = 8), and others (8%, n = 4).
Discussion
In this survey, we describe how the pandemic is undermining the education of residents in otolaryngology by reducing clinical and surgical opportunities. This was reflected in the procedures performed, with a significant decrease in flexible nasolaryngoscopy, rigid nasal endoscopy, and others. Furthermore, we believe that the most critical item affected is exposure to surgical opportunity; only 38% of the residents were involved in the operating room, and just 25% performed as the first surgeon for the entire month. We evaluated whether there was an association regarding the post-graduate year and being the first surgeon, but this was not significant (P = 0.0631). We believe that some of the factors that are possibly involved in the pandemic’s impact include the number of residents per hospital, mandatory quarantines depending on the city, and the population size for the different hospitals.
As it is uncertain when the pandemic will end, attention must be paid to provide residents with educational opportunities, especially regarding surgical skills. Some of the otolaryngology departments’ measures during April included videoconferences (bibliographical, case seminars, weekly journal clubs), bibliographical reviews, online surgical skills video analysis, and simulation opportunities.
At the moment our survey was completed, there were 65.393 cases[10]; we suspect that our activity level will be further affected as the peak of infection was in June. As many institutions arestill restricting outpatient clinics, we do not know how deeply this pandemic will impact our residency programs, we believe that measures should be taken by our sanitary authorities in order to insure a complete and proficient education of the current cohort of residents, also considering that otolaryngology is one of many surgical specialties that are most likely to be affected by the decrease in surgical cases.
We hereby describe the first experience showing an objective decrease in clinical and surgical activity secondary to the COVID-19 pandemic. There are concerns worldwide relating topostgraduate education and safety, Cai et al[11] performed a survey study evaluating 82 residents from 51 programs, and showed that 98% of the American programs enacted policy changesincluding a reduction in resident staffing surgeries, filtered respirator use for aerosol-generating procedures, and reduced frequency of tracheostomy care. Even though most of the residents surveyed felt satisfied with their department’s measures, they felt they were at greater risk than the attendants to get infected. However, procedures and surgeries performed were not evaluated.
This study’s limitations include the short period of evaluation (one month), lack of follow-up during the pandemic, and the lack of data regarding comparisons for functional endoscopic sinus surgery and head and neck oncology, because of incomplete data logs in those specific areas.
Conclusions
The COVID-19 pandemic is a new, aggressive, and long-lasting problem. There is no certainty regarding how deeply it will affect residency training. We show a sharp decrease in exposure to patients, procedures, and surgeries in otolaryngology. Further measures and close follow-up are required to cope with this ongoing adversity. Residency programs, with the support of the sanitary authorities, need to modify their current curricula to ensure resident safety and educational opportunities during the COVID-19 pandemic.
Notes
Appendix
Appendix: Survey “Education opportunities in the Otolaryngology training program during the COVID-19 Pandemic”.
Roles and contributions of authorship
MLA, SW, MT, PHD: conceptualization, methodology, data analysis, writing and critical review of the manuscript, final approval. CG, CN, RA, FF, RB: participated in conceptualization, methodology, writing and critical review of the manuscript, final approval.
Conflicts of interest
The authors declare that they have no competing interests.
Funding
Dr. Paul H Delano is funded by ANID Basal FB0008. Funding was also provided by the Otolaryngology Department of the Pontificia Universidad Católica de Chile.
Ethics approval
This study was approved by the Pontificia Universidad Católica de Chile Ethics Committee (protocol number: 200501001) on May 9, 2020.
Data analysis
The authors declare their willingness to share the study data upon request.
From the editors
The original version of this manuscript was submitted in Spanish. This English version was submitted by the authors and has been lightly copyedited by the Journal.

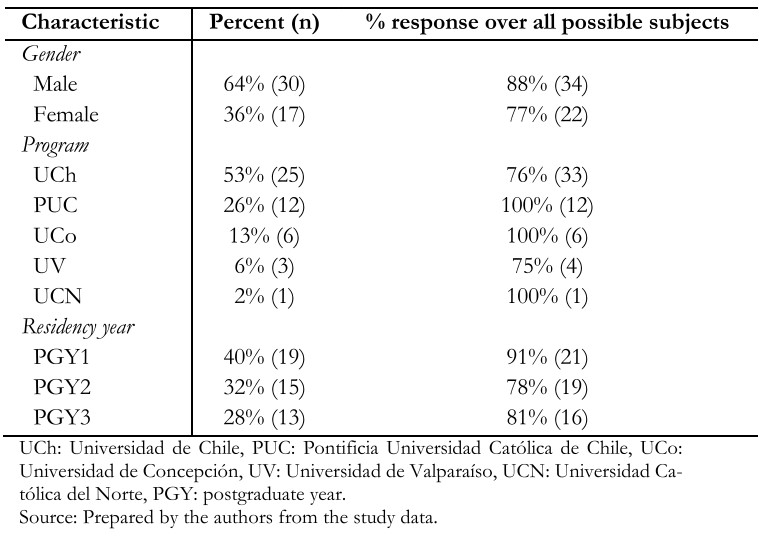 Table 1. Demographic data of otolaryngology head and neck surgery residents (n = 47).
Table 1. Demographic data of otolaryngology head and neck surgery residents (n = 47).
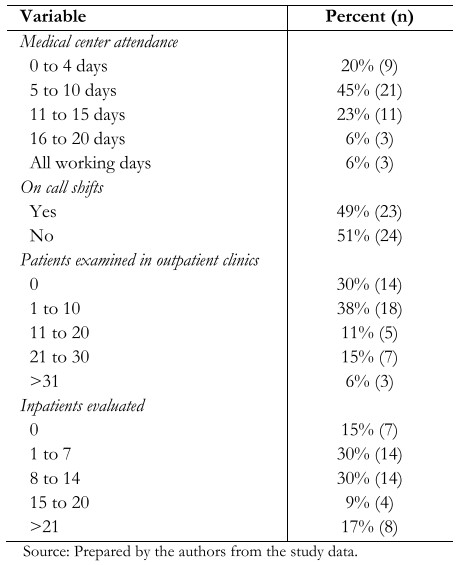 Table 2. Clinical activity level of otolaryngology head and neck surgery residents during April 2020 (n = 47).
Table 2. Clinical activity level of otolaryngology head and neck surgery residents during April 2020 (n = 47).
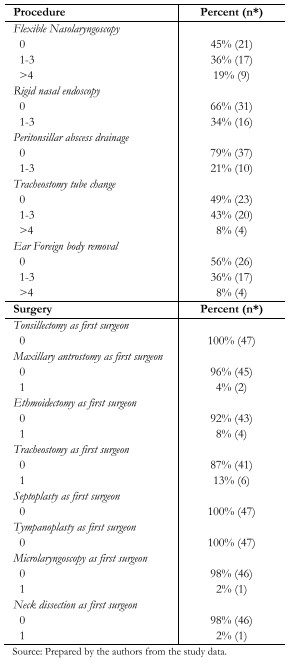 Table 3. Quantity of procedures and surgeries performed by the residents during April 2020.
Table 3. Quantity of procedures and surgeries performed by the residents during April 2020.
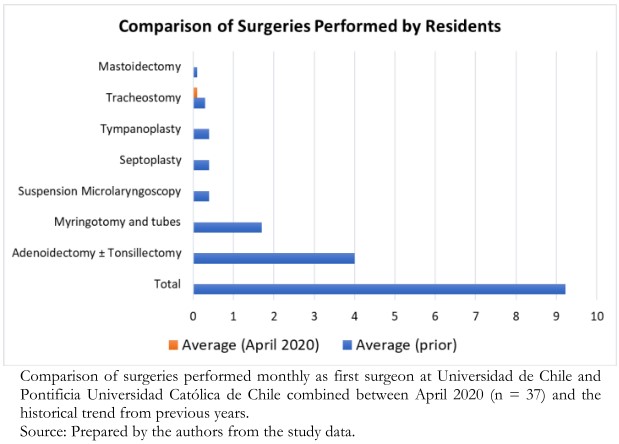 Figure 1. Comparison of Surgeries Performed by Residents.
Figure 1. Comparison of Surgeries Performed by Residents.
 Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
Introducción
La enfermedad por coronavirus 2019, o COVID-19, se ha convertido en una pandemia. Dada que la mayor carga viral de coronavirus de tipo 2 causante del síndrome respiratorio agudo severo (SARS-CoV-2) se encuentra en la vía aérea, los otorrinolaringólogos tienen un elevado riesgo de infección. Múltiples recomendaciones han surgido con respecto a las medidas de protección, incluidos la suspensión de procedimientos y cirugías electivas.
Objetivos
Evaluar el impacto de la pandemia de COVID-19 en los programas de formación de otorrinolaringología a nivel nacional.
Métodos
Estudio transversal de encuesta en línea a residentes de otorrinolaringología realizado durante abril de 2020. Se analizaron datos demográficos, actividades clínicas, turnos de llamado, infección por COVID-19, exposición a pacientes COVID-19 positivos, despliegue a otras especialidades, procedimientos y cirugías realizadas. Se utilizaron los portafolios quirúrgicos de ańos previos para comparar los resultados.
Resultados
Completaron la encuesta 47 residentes, con 84% de tasa de respuesta; el 64% refirió haber acudido a su centro asistencial 10 días o menos durante el mes de abril de 2020. Con relación a procedimientos frecuentes tales como nasofibroscopía, endoscopia nasal rígida y drenaje de absceso periamigdalino, no fueron realizados por más del 40% de los residentes en el mes. Solo el 38% participó en cirugías, con un promedio de 0,6 procedimientos como primer cirujano; se constata una drástica disminución al comparar los registros de ańos anteriores. La mayoría de los residentes refieren estas medidas educativas complementarias: videoconferencias bibliográficas (87%), seminarios de casos clínicos en línea (60%), revisión de artículos (38%), entre otros.
Conclusiones
La formación clínica y quirúrgica disminuyó drásticamente durante abril de 2020. Se deben considerar ajustes a los planes de estudio para disminuir el impacto negativo de la pandemia en la formación de los residentes.
Authors:
Matías L Álvarez[1], Sofia Waissbluth[1], Claudia González[1], Carla Napolitano[1], Mariela Torrente[2], Paul H Délano[3], Ricardo Alarcón[4], Francisca Fernández[5], Roger Bitrán[6]
Affiliation:
[1] Departamento Otorrinolaringología, Facultad de Medicina, Pontificia Universidad Católica de Chile, Santiago, Chile
[2] Departamento Otorrinolaringología, Facultad de Medicina, Universidad de Chile, Santiago, Chile
[3] Centro Avanzado de Ingeniería Eléctrica y Electrónica, AC3E, Universidad Técnica Federico Santa María, Valparaíso, Chile
[4] Departamento Otorrinolaringología, Facultad de Medicina, Universidad de Concepción, Concepción, Chile
[5] Departamento Otorrinolaringología, Facultad de Medicina, Universidad de Valparaíso, Valparaíso, Chile
[6] Departamento Otorrinolaringología, Facultad de Medicina, Universidad de Católica del Norte, Coquimbo, Chile
E-mail: sofia.waissbluth@gmail.com
Author address:
[1] Diagonal Paraguay 362, 7ş piso Santiago, Chile
Citation: Álvarez ML, Waissbluth S, González C, Napolitano C, Torrente M, Délano PH, et al. How the COVID-19 pandemic affects specialty training: An analysis of a nationwide survey among otolaryngology residents in Chile. Medwave 2021;21(1):e8097 doi: 10.5867/medwave.2021.01.8097
Submission date: 29/8/2020
Acceptance date: 20/10/2020
Publication date: 8/1/2021
Origin: Not commissioned
Type of review: Externally peer-reviewed by five reviewers, double-blind
Comments (0)
We are pleased to have your comment on one of our articles. Your comment will be published as soon as it is posted. However, Medwave reserves the right to remove it later if the editors consider your comment to be: offensive in some sense, irrelevant, trivial, contains grammatical mistakes, contains political harangues, appears to be advertising, contains data from a particular person or suggests the need for changes in practice in terms of diagnostic, preventive or therapeutic interventions, if that evidence has not previously been published in a peer-reviewed journal.
No comments on this article.
To comment please log in
Medwave provides HTML and PDF download counts as well as other harvested interaction metrics. There may be a 48-hour delay for most recent metrics to be posted.
- Zhu W, Xie K, Lu H, Xu L, Zhou S, Fang S. Initial clinical features of suspected coronavirus disease 2019 in two emergency departments outside of Hubei, China. J Med Virol. 2020 Sep;92(9):1525-1532. | CrossRef | PubMed |
- Zou L, Ruan F, Huang M, Liang L, Huang H, Hong Z, et al. SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients. N Engl J Med. 2020 Mar 19;382(12):1177-1179. | CrossRef | PubMed |
- van Doremalen N, Bushmaker T, Morris DH, Holbrook MG, Gamble A, Williamson BN, et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N Engl J Med. 2020 Apr 16;382(16):1564-1567. | CrossRef | PubMed |
- Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7(4):e35797. | CrossRef | PubMed |
- Givi B, Schiff BA, Chinn SB, Clayburgh D, Iyer NG, Jalisi S, et al. Safety Recommendations for Evaluation and Surgery of the Head and Neck During the COVID-19 Pandemic. JAMA Otolaryngol Head Neck Surg. 2020 Jun 1;146(6):579-584. | CrossRef | PubMed |
- Wu V, Noel CW, Forner D, Zhang ZJ, Higgins KM, Enepekides DJ, et al. Considerations for head and neck oncology practices during the coronavirus disease 2019 (COVID-19) pandemic: Wuhan and Toronto experience. Head Neck. 2020 Jun;42(6):1202-1208. | CrossRef | PubMed |
- Rameau A, Young VN, Amin MR, Sulica L. Flexible Laryngoscopy and COVID-19. Otolaryngol Head Neck Surg. 2020 Jun;162(6):813-815. | CrossRef | PubMed |
- Maza-Solano JM, Plaza-Mayor G, Jiménez-Luna A, Parente-Arias P, Amor-Dorado JC. Strategies for the practice of otolaryngology and head and neck surgery during the monitoring phase of COVID-19. Acta Otorrinolaringol Esp. 2020 Nov-Dec;71(6):367-378. | CrossRef | PubMed |
- Crosby DL, Sharma A. Insights on Otolaryngology Residency Training during the COVID-19 Pandemic. Otolaryngol Head Neck Surg. 2020 Jul;163(1):38-41. | CrossRef | PubMed |
- Gobierno de Chile , Ministerio de Salud. Casos confirmados en Chile COVID-19. Santiago: MINSAL, 2020. [On line]. | Link |
- Cai Y, Jiam NT, Wai KC, Shuman EA, Roland LT, Chang JL. Otolaryngology Resident Practices and Perceptions in the Initial Phase of the U.S. COVID-19 Pandemic. Laryngoscope. 2020 Nov;130(11):2550-2557. | CrossRef | PubMed |
Zhu W, Xie K, Lu H, Xu L, Zhou S, Fang S. Initial clinical features of suspected coronavirus disease 2019 in two emergency departments outside of Hubei, China. J Med Virol. 2020 Sep;92(9):1525-1532. | CrossRef | PubMed |Zou L, Ruan F, Huang M, Liang L, Huang H, Hong Z, et al. SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients. N Engl J Med. 2020 Mar 19;382(12):1177-1179. | CrossRef | PubMed |van Doremalen N, Bushmaker T, Morris DH, Holbrook MG, Gamble A, Williamson BN, et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N Engl J Med. 2020 Apr 16;382(16):1564-1567. | CrossRef | PubMed |Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7(4):e35797. | CrossRef | PubMed |Givi B, Schiff BA, Chinn SB, Clayburgh D, Iyer NG, Jalisi S, et al. Safety Recommendations for Evaluation and Surgery of the Head and Neck During the COVID-19 Pandemic. JAMA Otolaryngol Head Neck Surg. 2020 Jun 1;146(6):579-584. | CrossRef | PubMed |Wu V, Noel CW, Forner D, Zhang ZJ, Higgins KM, Enepekides DJ, et al. Considerations for head and neck oncology practices during the coronavirus disease 2019 (COVID-19) pandemic: Wuhan and Toronto experience. Head Neck. 2020 Jun;42(6):1202-1208. | CrossRef | PubMed |Rameau A, Young VN, Amin MR, Sulica L. Flexible Laryngoscopy and COVID-19. Otolaryngol Head Neck Surg. 2020 Jun;162(6):813-815. | CrossRef | PubMed |Maza-Solano JM, Plaza-Mayor G, Jiménez-Luna A, Parente-Arias P, Amor-Dorado JC. Strategies for the practice of otolaryngology and head and neck surgery during the monitoring phase of COVID-19. Acta Otorrinolaringol Esp. 2020 Nov-Dec;71(6):367-378. | CrossRef | PubMed |Crosby DL, Sharma A. Insights on Otolaryngology Residency Training during the COVID-19 Pandemic. Otolaryngol Head Neck Surg. 2020 Jul;163(1):38-41. | CrossRef | PubMed |Gobierno de Chile , Ministerio de Salud. Casos confirmados en Chile COVID-19. Santiago: MINSAL, 2020. [On line]. | Link |





 Research papers
Research papersSystematization of initiatives in sexual and reproductive health about good practices criteria in response to the COVID-19 pandemic in primary health care in Chile
Clinical, psychological, social, and family characterization of suicidal behavior in Chilean adolescents: a multiple correspondence analysis
