
Key Words: chemo-mechanical caries removal, caries removal, dental caries, minimally invasive dentistry, Epistemonikos, GRADE.
Abstract
INTRODUCTION
Dental caries have been traditionally managed with the non-selective removal of carious tissue (total removal). However, the adverse effects and fear that this technique produces in patients has promoted the use of more conservative caries removal techniques such as chemo-mechanical removal, but there is still controversy regarding its effectiveness and safety.
METHODS
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings tables using the GRADE approach.
RESULTS AND CONCLUSIONS
We identified seven systematic reviews including 34 studies overall, of which 30 correspond to randomized trials. We concluded that chemo-mechanical caries removal probably reduces the need for anesthesia. Additionally, chemo-mechanical caries removal may decrease the pain experienced by the patient, decrease the risk of restoration failure and increase the time of the procedure for the removal of deep caries, but the certainty of the evidence is low. We are uncertain whether chemo-mechanical caries removal reduces the risk of pulp exposure as the certainty of the evidence has been assessed as very low.
Problem
Dental caries, the most prevalent oral condition worldwide [1], produces localized destruction of dental tissue [2]. The treatment of carious lesions consists of their removal and subsequent restorative treatment.
Currently there are several techniques for tooth decay removal. Conventional treatment involves the total (non-selective) removal of the caries with rotary and manual instruments. In recent years, the total removal technique has been criticized for increasing the risk of pulp exposure and pulp diseases [3], [4].
In addition, the conventional total removal technique causes anxiety and fear in patients. Consequently, new alternatives for caries removal have emerged such as chemo-mechanical removal [5], which allows the removal of carious tissue through the application of a substance that softens the affected tissue in combination with manual instrumentation [6]. The most reported products in the literature to carry out this technique are Carisolv (swedish origin) and Papacarie (brazil origin). Its mechanism of action is comparable and is based on the breakdown of partially degraded collagen molecules, which contributes to the degradation and elimination of the fibrin mantle formed by the carious process [7], [8]. However, it has been suggested that this technique would lead to restoration failure, so its use remains controversial [9]. This summary aims to evaluate the effectiveness and safety of chemo-mechanical removal compared to conventional total caries removal.
Methods
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We identified seven systematic reviews [9], [10], [11], [12], [13], [14], [15] including 34 primary studies reported in 35 references [16], [17], [18], [19], [20], [21], [22], [23], [24], [25], [26], [27], [28], [29], [30], [31], [32], [33], [34], [35], [36], [37], [38], [39], [40], [41], [42], [43], [44], [45], [46], [47], [48], [49], of which 30 were randomized trials [16], [17], [18], [19], [20], [21], [22], [23], [24], [25], [27], [28], [30], [31], [32], [33], [35], [36], [37], [38], [39], [40], [41], [42], [43], [45], [46], [47], [48, [49]. The table and summary are based on the randomized trials, as the observational studies did not increase the level of certainty of the evidence, nor added any additional relevant information. |
|
What types of patients were included* |
Of the 30 trials, 20 included only children (two to 12 years) [18], [19], [20], [21], [22], [23], [24], [27], [30], [31], [33], [35], [36], [37], [38], [40], [43], [46], [47], [49], four trials included children and adults (2.5 to 85 years) [16], [25], [28], [41], four trials included children, adolescents and adults (six to 68 years) [17], [39], [42], [48] and two trials did not report the age of the participants [32], [45]. Nineteen trials included only primary teeth [18], [19], [20], [21], [22], [23], [24], [27], [30], [31], [33], [36], [37], [38], [43], [45], [46], [47], [49], four trials included only permanent teeth [17], [39], [42], [48], four trials both dentitions [16], [25], [28], [41] and three trials did not report the type of dentition [32], [35], [40]. Finally, regarding the extent of the caries, all included only dentin caries, excluding those lesions limited only to enamel. [16], [17], [18], [19], [20], [21], [22], [23], [24], [25], [27], [28], [30], [31], [32], [33], [35], [36], [37], [38], [39], [40], [41], [42], [43], [45], [46], [47], [48]. |
|
What types of interventions were included* |
All trials compared chemo-mechanical removal against conventional treatment (total removal). Chemo-mechanical removal was described differently by the trials, but in general it was defined as the removal of cavities using chemicals that degrade carious tissue (Carisolv, Caridex, Carie-care or Papacarie) followed by the removal of the softened tissue with mechanical removal (spoon excavator) [9]. Fourteen trials used Carisolv [16], [17], [21], [24], [25], [27], [28], [30], [31], [41], [43], [45], [47], [48]. Seven trials used Papacarie [19], [20], [22], [23], [33], [40], [49]. Three studies compared Carisolv and Papacarie [18], [35], [46]. Four studies [36], [37], [38], [39] report using the Carie-care material. A single trial [32] used Caridex and only one trial [42] did not report what type of material was used. Total removal was described as excavation until pulpo-proximal dentine on the cavity floor was hard on probing [9]. |
|
What types of outcomes |
The trials evaluated multiple outcomes, which were grouped by the systematic reviews as follows:
These trials reported [22,33,24,25,33,47] follow-up that ranged from 1 to 18 months; the other studies did not report the follow-up time. |
* Information about primary studies is not extracted directly from primary studies but from identified systematic reviews, unless otherwise stated.
Summary of findings
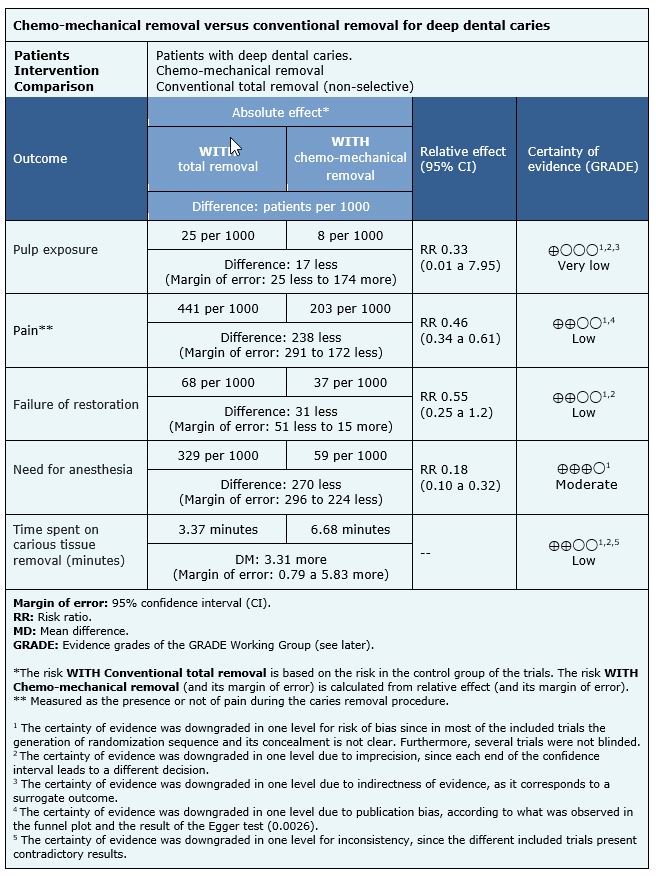
Only one trial measured pulp exposure events (40 patients, 80 teeth) [30], 10 trials measured pain (553 patients and 839 teeth) [16], [20], [22], [24], [25], [28], [31], [38], [47], [48], six trials evaluated restoration failure events (261 patients, 432 teeth) [21], [22], [24], [25], [31], [47], 14 trials measured the need for anesthesia (703 patients and 1169 teeth) [16], [17], [21], [23], [24], [25], [28], [30], [31], [32], [33], [39], [47], [48] and 24 trials measured time spent on carious tissue removal (1163 patients and 2069 teeth) [16], [17], [18], [19], [20], [21], [22], [23], [24], [25], [27], [28], [30], [31], [32], [33], [35], [36], [37], [38], [39], [46], [47], [48].
The summary of findings is as follows:
- We are uncertain whether chemo-mechanical caries removal reduces the risk of pulp exposure as the certainty of the evidence has been assessed as very low.
- Chemo-mechanical caries removal compared to total removal may decrease the risk of pain during caries removal procedure (low certainty of evidence).
- Chemo-mechanical caries removal compared to conventional total removal may decrease the risk of failure of restorations (low certainty of evidence).
- Chemo-mechanical caries removal compared to conventional total removal probably reduces the need for anesthesia (moderate certainty evidence).
- Chemo-mechanical caries removal compared to conventional total removal could increase the time of the procedure (low certainty of the evidence).
| Follow the link to access the interactive version of this table (Interactive Summary of Findings – iSoF) |

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
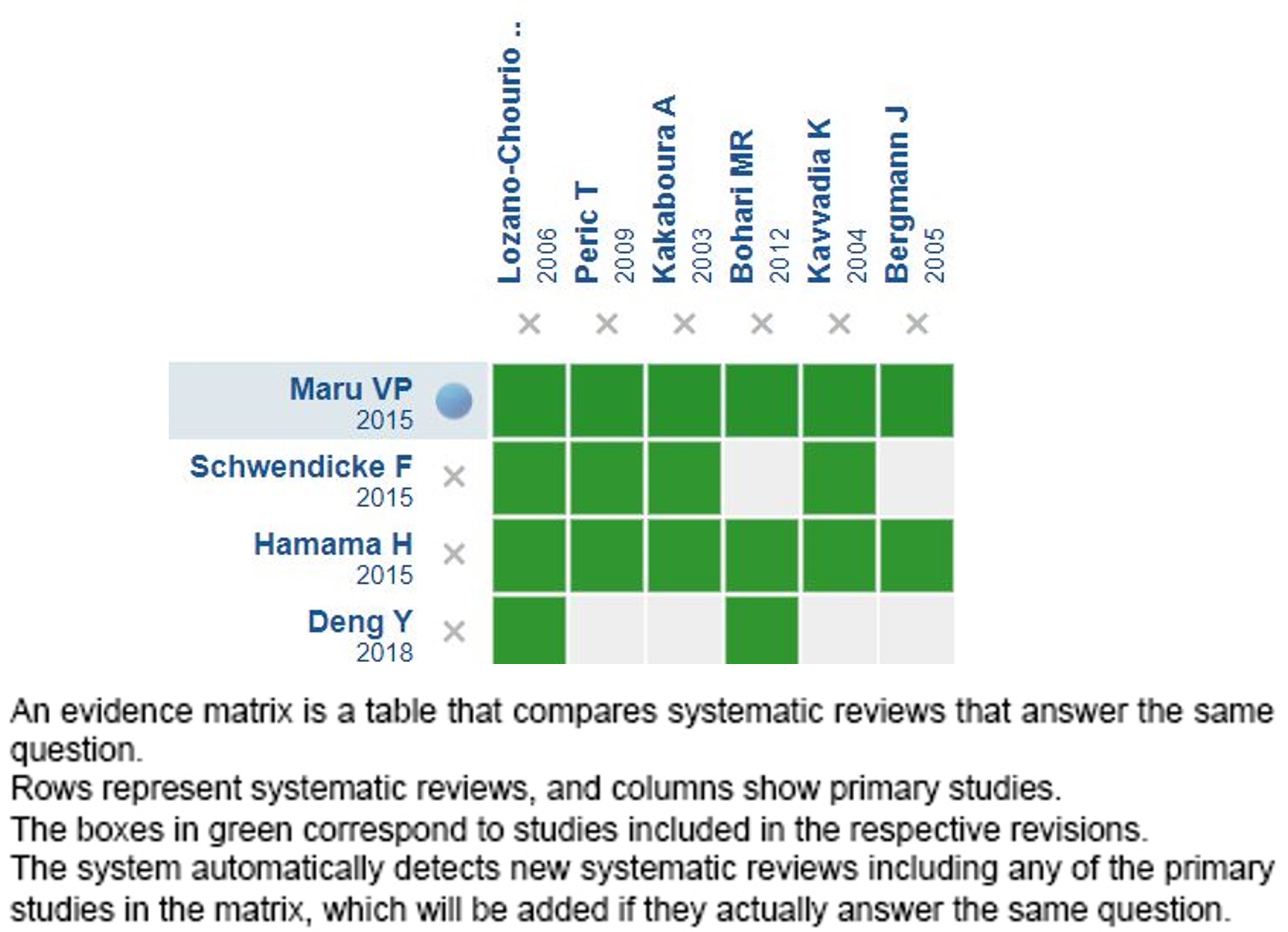
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
Follow the link to access the interactive version: Chemo-mechanical removal versus conventional removal for deep dental caries
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.


INTRODUCCION
La caries dental tradicionalmente es manejada con la remoción no selectiva del tejido carioso (remoción total). Sin embargo, los efectos adversos y el temor que produce esta técnica en los pacientes ha promovido la utilización de técnicas de remoción de caries más conservadoras como la remoción químico-mecánica, pero aún existe controversia respecto a su efectividad y seguridad.
MÉTODOS
Para responder esta pregunta utilizamos Epistemonikos, la mayor base de datos de revisiones sistemáticas en salud, la cual es mantenida mediante búsquedas en múltiples fuentes de información, incluyendo MEDLINE, EMBASE, Cochrane Library, entre otras. Extrajimos los datos desde las revisiones identificadas, analizamos los datos de los estudios primarios, realizamos un metaanálisis y preparamos tablas de resumen de los resultados utilizando el método GRADE.
RESULTADOS Y CONCLUSIONES
Identificamos siete revisiones sistemáticas que en conjunto incluyeron 34 estudios primarios, de los cuales 30 corresponden a ensayos aleatorizados. Concluimos que la remoción químico-mecánica de caries probablemente disminuye la necesidad de anestesia. Además, podría disminuir el dolor que experimenta el paciente, disminuir el riesgo del fracaso de la restauración y aumentar el tiempo del procedimiento, pero la certeza de la evidencia es baja. No es posible establecer con claridad si la remoción químico- mecánica disminuye el riesgo de exposición pulpar debido a que la certeza de la evidencia existente ha sido evaluada como muy baja.
Authors:
Paula Zambrano-Achig[1,2], Andrés Viteri-García[1,2], Francisca Verdugo-Paiva[2,3]
Affiliation:
[1] Centro Evidencia UC Pontificia Universidad Católica de Chile Diagonal Paraguay 476 Santiago Chile
Citation: Zambrano-Achig , Viteri-García , Verdugo-Paiva . . 2022;22(01):e8319 doi: 10.5867/medwave.2022.01.8319
Submission date: 5/5/2020
Acceptance date: 15/1/2021
Publication date: 28/1/2022
Origin: Este artículo es producto del Epistemonikos Evidence Synthesis Project de la Fundación Epistemonikos, en colaboración con Medwave para su publicación.
Type of review: Con revisión por pares sin ciego por parte del equipo metodológico del Centro Evidencia UC Synthesis Project
Comments (0)
We are pleased to have your comment on one of our articles. Your comment will be published as soon as it is posted. However, Medwave reserves the right to remove it later if the editors consider your comment to be: offensive in some sense, irrelevant, trivial, contains grammatical mistakes, contains political harangues, appears to be advertising, contains data from a particular person or suggests the need for changes in practice in terms of diagnostic, preventive or therapeutic interventions, if that evidence has not previously been published in a peer-reviewed journal.
No comments on this article.
To comment please log in
Medwave provides HTML and PDF download counts as well as other harvested interaction metrics. There may be a 48-hour delay for most recent metrics to be posted.
- Petersen P, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bull World Heal Organ. 2005;83(9):661–9.
- Roberson TM, Heymann H, Swift EJ, Sturdevant CM. Sturdevant’s Art and science of operative dentistry. 2002. 60–128 p.
- White J, Eakle W. Rationale and treatment approach in minimally invasive dentistry. J Am Dent Assoc. 2000;131.
- Banerjee A. Minimal intervention dentistry: part 7. Minimally invasive operative caries management: rationale and techniques. Br Dent J. 2013;214(3):107–11.
- Armfi J, Spencer A. Changes in South Australian children’s caries experience: is caries re-surfacing? Aust Dent J. 2004;49(4):2–12.
- Yip H, Stevenson A, Beeley A. Chemomechanical removal of dental caries in deciduous teeth: further studies in vitro. BDJ. 1999;186(4):179–82.
- Goldman M, Kronman J. A preliminary report on a chemomechanical means of removing caries. J Am Dent Assoc. 1976;93(6):1149–53.
- Doglas C, Ana F, Franciele O, Eloisa B, Bruno C. Effect of Carisolv and Papacarie on the resin dentin bond strength in sound and caries affected primary molars. Braz J Oral Sci. 2010;9:25–9.
- Schwendicke F, Paris S, Tu Y. Effects of using different criteria for caries removal: a systematic review and network meta-analysis. J Dent. 2015;43(1):1–15.
- Lai G, Lara Capi C, Cocco F, Cagetti MG, Lingstrom P, Almhojd U, et al. Comparison of Carisolv system vs traditional rotating instruments for caries removal in the primary dentition: A systematic review and meta-analysis. Acta Odontol Scand. 2015;73(8):569–80.
- Li R, Zhao Y, Ye L. How to make choice of the carious removal methods, Carisolv or traditional drilling? A meta-analysis. J Oral Rehabil. 2014.
- Maru VP, Shakuntala, B.S. Nagarathna C. Caries Removal by Chemomechanical (CarisolvTM) vs. Rotary Drill: A Systematic Review. Dent J. 2015;9:462–72.
- Deng Y, Feng G, Hu B, Kuang Y, Song J. Effects of Papacarie on children with dental caries in primary teeth: a systematic review and meta-analysis. Int J Paediatr Dent. 2018.
- Hamama H, Yiu C, Burrow M, King N. Systematic Review and Meta-Analysis of Randomized Clinical Trials on Chemomechanical Caries Removal. Oper Dent. 2015;40(4):167–78.
- Yun J, Shim Y-S, Park S-Y, An S-Y. New treatment method for pain and reduction of local anesthesia use in deep caries. J Dent Anesth Pain Med. 2018;18(5):277–85.
- Balciuniene I, Sabalaite R, Juskiene I. Chemomechanical caries removal for children. Stomatologija. 2005;7(2):40–4.
- Kakaboura A, Masouras C, Staikou O, Vougiouklakis G. A comparative clinical study on the Carisolv caries removal method. Quintessence Int (Berl). 2003;34(4):269–71.
- Bohari M, Chunawalla Y, Ahmed B. Clinical evaluation of caries removal in primary teeth using conventional chemomechanical and laser technique: An in vivo study. J Contemp Dent Pr. 2012;13(1):40–7.
- Singh S, Singh DJ, Jaidka S, Somani R. Comparative clinical evaluation of chemomechanical caries removal agent Papacarie® with conventional method among rural population in India - in vivo study Sanjeet Singh. Brazilian J Oral Sci. 2011;10(3).
- Anegundi R, Patil S, Tegginmani V, Shetty S. A comparative microbiological study to assess caries excavation by conventional rotary method and a chemo-mechanical method. Contemp Clin Dent. 2012;3(4):388–92.
- Kavvadia K, Karagianni V, Polychronopoulou A, Papagiannouli L. Primary teeth caries removal using the Carisolv chemomechanical method: a clinical trial. Pediatr Dent. 2004;26(1):23–8.
- Matsumoto S, Motta L, Alfaya T, Guedes C, Fernandes K, Bussadori SK. Assessment of chemomechanical removal of carious lesions using Papacarie Duo: randomized longitudinal clinical trial. Indian J Dent Res. 2013;24(4):488–492.
- Kotb R, Abdella A, El Kateb M, Ahmed A. Clinical evaluation of Papacarie in primary teeth. J Clin Pediatr Dent. 2009;34(2):117–23.
- Bergmann J, Leităo J, Kultje C, Bergmann D, Joăo C. Removing dentine caries in deciduous teeth with Carisolv: A randomised, controlled, prospective study with six-month follow-up, comparing chemomechanical treatment with drilling. Oral Health Prev Dent. 2005;3(2):105–11.
- Peric T, Markovic D, Petrovic B. Clinical evaluation of a chemomechanical method for caries removal in children and adolescents. Acta Odontol Scand. 2009;67(5):277–28.
- Peters M, Flamenbaum M, Eboda N, Feigal R, Inglehart M. Chemomechanical caries removal in children: Efficacy and efficiency. J Am Dent Assoc. 2006;137(12):1658–66.
- Goomer P, Jain R, Kaur H, Sood R. Comparison of the efficacy of chemicomechanical caries removal with conventional methods: A clinical study. J Int Oral Heal. 2013;5(3):42–7.
- Ericson D, Zimmerman M, Raber H, Gotrick B, Bornstein R, Thorell J. Clinical evaluation of efficacy and safety of a new method for chemo-mechanical removal of caries. A multi-centre study. Caries Res. 1999;33(3):171–7.
- Inglehart M, Peters M, Flamenbaum M, Eboda N, Feigal R. Chemomechanical caries removal in children: an operator’s and pediatric patients’ responses. J Am Dent Assoc. 2007;138(1):47–55.
- Lozano-Chourio MA, Zambrano O, Gonzalez H, Quero M. Clinical randomized controlled trial of chemomechanical caries removal (Carisolv). Int J Paediatr Dent. 2006 May;16(3):161–7.
- Maragakis G, Hahn P, Hellwig E. Clinical evaluation of chemomechanical caries removal in primary molars and its acceptance by patients. Caries Res. 2001;35(3):205–10.
- Zinck J, McInnes-Ledoux, P Capdeboscq C, Weinberg R. Chemomechanical caries removal – a clinical evaluation. J Oral Rehab. 1988;15(1):23–33.
- Motta L, Bussadori S, Campanelli A, da Silva A, Alfaya T, de Godoy C. Pain during removal of carious lesions in children: a randomized controlled clinical trial. Int J Dent. 2013.
- Hosein T, Hasan A. Efficacy of chemo mechanical caries removal with Carisolv. J Coll Physicians Surg Pakistan. 2008;18(4):222–5.
- Hegde S, Kakti A, Bolar D, Bhaskar S. Clinical Efficiency of Three Caries Removal Systems: Rotary Excavation, Carisolv, and Papacarie. J Dent Child. 2016;83(1):22–8.
- Rajakumar S, Mungara J, Joseph E, Philip J, Shilpa, Priya M. Evaluation of three different caries removal techniques in children: a comparative clinical study. J Clin Pediatr Dent. 2013;38(1):23–6.
- Hegde R, Chaudhari S. Comparative evaluation of mechanical and chemo-mechanical methods of caries excavation: an in vivo study. J Int Oral Heal. 2016;8:357–61.
- Nagaveni N, Radhika N, Satisha T, Ashwini K, Neni S, Gupta S. Efficacy of new chemomechanical caries removal agent compared with conventional method in primary teeth: An in vivo study. Int J Oral Health Sci. 2016;6:52–8.
- Pathivada L, Krishna M, Kalra M, Ivekanandan G, Singh J, Navit S. Clinical evaluation of a papain-based gel for the chemo-mechanical removal of caries in children. Oral Heal Dent Manag. 2016;15:145–9.
- Goyal P, Kumari R, Kannan V, Madhu S. Efficacy and tolerance of papain gel with conventional drilling method: a clinico-microbiological study. J Clin Pediatr Dent. 2015;39(2):109–12.
- Soni HK, Sharma A, Sood PB. A comparative clinical study of various methods of caries removal in children. Eur Arch Paediatr Dent. 2015 Feb;16(1):19–26.
- Lager A, Thornqvist E, Ericson D. Cultivatable bacteria in dentine after caries excavation using rose-bur or carisolv. Caries Res. 2003;37(3):206–11.
- Azrak B, Callaway A, Grundheber A, Stender E, Willershausen B. Comparison of the efficacy of chemomechanical caries removal (Carisolv) with that of conventional excavation in reducing the cariogenic flora. Int J Paediatr Dent. 2004;14(3):182–91.
- Pandit I, Srivastava N, Gugnani N, Gupta M VL. Various methods of caries removal in children: A comparative clinical study. J Ind Soc Pedod Prev Dent. 2007;25(2):93–6.
- Subramaniam P, Babu K, Neeraja G. Comparison of the antimicrobial efficacy of chemomechanical caries removal (Carisolv) with that of conventional drilling in reducing cariogenic flora. J Clin Pediatr Dent. 2008;32(3):215–9.
- Kochhar GK, Srivastava N, Pandit IK, Gugnani N GM. An evaluation of different caries removal techniques in primary teeth: a comparitive clinical study. J Clin Pediatr Dent. 2011;36(1):5–9.
- Kirzioglu Z, Gurbuz T, Yilmaz Y. Clinical evaluation of chemomechanical and mechanical caries removal: status of the restorations at 3, 6, 9 and 12 months. Clin Oral Investig. 2007 Mar;11(1):69–76.
- Nadanovsky P, Cohen Carneiro F, Souza de Mello F. Removal of caries using only hand instruments: a comparison of mechanical and chemo-mechanical methods. Caries Res. 2001;35(5):384–9.
- Maru VP, Kumar A, Badiyani BK, Sharma AR, Sharma J, Dobariya CV. Behavioral changes in preschoolers treated with/without rotary instruments. J Int Soc Prev Community Dent. 2014 May;4(2):77–81.
- Schwendicke F, Frencken J, Bjřrndal L, Maltz M, Manton D, Ricketts D, et al. Managing Carious Lesions: Consensus Recommendations on Carious Tissue Removal. Adv Dent Res. 2016;28(2):58–67.
- NCT01641861. A Comparative study of Papacarie and the Conventional Method for dental caries treatment. | Link |
- NCT01811420. Chemomechanical caries removal using papain gel ( CMCR09) | Link |
Petersen P, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bull World Heal Organ. 2005;83(9):661–9. Roberson TM, Heymann H, Swift EJ, Sturdevant CM. Sturdevant’s Art and science of operative dentistry. 2002. 60–128 p. White J, Eakle W. Rationale and treatment approach in minimally invasive dentistry. J Am Dent Assoc. 2000;131. Banerjee A. Minimal intervention dentistry: part 7. Minimally invasive operative caries management: rationale and techniques. Br Dent J. 2013;214(3):107–11. Armfi J, Spencer A. Changes in South Australian children’s caries experience: is caries re-surfacing? Aust Dent J. 2004;49(4):2–12. Yip H, Stevenson A, Beeley A. Chemomechanical removal of dental caries in deciduous teeth: further studies in vitro. BDJ. 1999;186(4):179–82. Goldman M, Kronman J. A preliminary report on a chemomechanical means of removing caries. J Am Dent Assoc. 1976;93(6):1149–53. Doglas C, Ana F, Franciele O, Eloisa B, Bruno C. Effect of Carisolv and Papacarie on the resin dentin bond strength in sound and caries affected primary molars. Braz J Oral Sci. 2010;9:25–9. Schwendicke F, Paris S, Tu Y. Effects of using different criteria for caries removal: a systematic review and network meta-analysis. J Dent. 2015;43(1):1–15. Lai G, Lara Capi C, Cocco F, Cagetti MG, Lingstrom P, Almhojd U, et al. Comparison of Carisolv system vs traditional rotating instruments for caries removal in the primary dentition: A systematic review and meta-analysis. Acta Odontol Scand. 2015;73(8):569–80. Li R, Zhao Y, Ye L. How to make choice of the carious removal methods, Carisolv or traditional drilling? A meta-analysis. J Oral Rehabil. 2014. Maru VP, Shakuntala, B.S. Nagarathna C. Caries Removal by Chemomechanical (CarisolvTM) vs. Rotary Drill: A Systematic Review. Dent J. 2015;9:462–72. Deng Y, Feng G, Hu B, Kuang Y, Song J. Effects of Papacarie on children with dental caries in primary teeth: a systematic review and meta-analysis. Int J Paediatr Dent. 2018. Hamama H, Yiu C, Burrow M, King N. Systematic Review and Meta-Analysis of Randomized Clinical Trials on Chemomechanical Caries Removal. Oper Dent. 2015;40(4):167–78. Yun J, Shim Y-S, Park S-Y, An S-Y. New treatment method for pain and reduction of local anesthesia use in deep caries. J Dent Anesth Pain Med. 2018;18(5):277–85. Balciuniene I, Sabalaite R, Juskiene I. Chemomechanical caries removal for children. Stomatologija. 2005;7(2):40–4. Kakaboura A, Masouras C, Staikou O, Vougiouklakis G. A comparative clinical study on the Carisolv caries removal method. Quintessence Int (Berl). 2003;34(4):269–71. Bohari M, Chunawalla Y, Ahmed B. Clinical evaluation of caries removal in primary teeth using conventional chemomechanical and laser technique: An in vivo study. J Contemp Dent Pr. 2012;13(1):40–7. Singh S, Singh DJ, Jaidka S, Somani R. Comparative clinical evaluation of chemomechanical caries removal agent Papacarie® with conventional method among rural population in India - in vivo study Sanjeet Singh. Brazilian J Oral Sci. 2011;10(3). Anegundi R, Patil S, Tegginmani V, Shetty S. A comparative microbiological study to assess caries excavation by conventional rotary method and a chemo-mechanical method. Contemp Clin Dent. 2012;3(4):388–92. Kavvadia K, Karagianni V, Polychronopoulou A, Papagiannouli L. Primary teeth caries removal using the Carisolv chemomechanical method: a clinical trial. Pediatr Dent. 2004;26(1):23–8. Matsumoto S, Motta L, Alfaya T, Guedes C, Fernandes K, Bussadori SK. Assessment of chemomechanical removal of carious lesions using Papacarie Duo: randomized longitudinal clinical trial. Indian J Dent Res. 2013;24(4):488–492. Kotb R, Abdella A, El Kateb M, Ahmed A. Clinical evaluation of Papacarie in primary teeth. J Clin Pediatr Dent. 2009;34(2):117–23. Bergmann J, Leităo J, Kultje C, Bergmann D, Joăo C. Removing dentine caries in deciduous teeth with Carisolv: A randomised, controlled, prospective study with six-month follow-up, comparing chemomechanical treatment with drilling. Oral Health Prev Dent. 2005;3(2):105–11. Peric T, Markovic D, Petrovic B. Clinical evaluation of a chemomechanical method for caries removal in children and adolescents. Acta Odontol Scand. 2009;67(5):277–28. Peters M, Flamenbaum M, Eboda N, Feigal R, Inglehart M. Chemomechanical caries removal in children: Efficacy and efficiency. J Am Dent Assoc. 2006;137(12):1658–66. Goomer P, Jain R, Kaur H, Sood R. Comparison of the efficacy of chemicomechanical caries removal with conventional methods: A clinical study. J Int Oral Heal. 2013;5(3):42–7. Ericson D, Zimmerman M, Raber H, Gotrick B, Bornstein R, Thorell J. Clinical evaluation of efficacy and safety of a new method for chemo-mechanical removal of caries. A multi-centre study. Caries Res. 1999;33(3):171–7. Inglehart M, Peters M, Flamenbaum M, Eboda N, Feigal R. Chemomechanical caries removal in children: an operator’s and pediatric patients’ responses. J Am Dent Assoc. 2007;138(1):47–55. Lozano-Chourio MA, Zambrano O, Gonzalez H, Quero M. Clinical randomized controlled trial of chemomechanical caries removal (Carisolv). Int J Paediatr Dent. 2006 May;16(3):161–7. Maragakis G, Hahn P, Hellwig E. Clinical evaluation of chemomechanical caries removal in primary molars and its acceptance by patients. Caries Res. 2001;35(3):205–10. Zinck J, McInnes-Ledoux, P Capdeboscq C, Weinberg R. Chemomechanical caries removal – a clinical evaluation. J Oral Rehab. 1988;15(1):23–33. Motta L, Bussadori S, Campanelli A, da Silva A, Alfaya T, de Godoy C. Pain during removal of carious lesions in children: a randomized controlled clinical trial. Int J Dent. 2013. Hosein T, Hasan A. Efficacy of chemo mechanical caries removal with Carisolv. J Coll Physicians Surg Pakistan. 2008;18(4):222–5. Hegde S, Kakti A, Bolar D, Bhaskar S. Clinical Efficiency of Three Caries Removal Systems: Rotary Excavation, Carisolv, and Papacarie. J Dent Child. 2016;83(1):22–8. Rajakumar S, Mungara J, Joseph E, Philip J, Shilpa, Priya M. Evaluation of three different caries removal techniques in children: a comparative clinical study. J Clin Pediatr Dent. 2013;38(1):23–6. Hegde R, Chaudhari S. Comparative evaluation of mechanical and chemo-mechanical methods of caries excavation: an in vivo study. J Int Oral Heal. 2016;8:357–61. Nagaveni N, Radhika N, Satisha T, Ashwini K, Neni S, Gupta S. Efficacy of new chemomechanical caries removal agent compared with conventional method in primary teeth: An in vivo study. Int J Oral Health Sci. 2016;6:52–8. Pathivada L, Krishna M, Kalra M, Ivekanandan G, Singh J, Navit S. Clinical evaluation of a papain-based gel for the chemo-mechanical removal of caries in children. Oral Heal Dent Manag. 2016;15:145–9. Goyal P, Kumari R, Kannan V, Madhu S. Efficacy and tolerance of papain gel with conventional drilling method: a clinico-microbiological study. J Clin Pediatr Dent. 2015;39(2):109–12. Soni HK, Sharma A, Sood PB. A comparative clinical study of various methods of caries removal in children. Eur Arch Paediatr Dent. 2015 Feb;16(1):19–26. Lager A, Thornqvist E, Ericson D. Cultivatable bacteria in dentine after caries excavation using rose-bur or carisolv. Caries Res. 2003;37(3):206–11. Azrak B, Callaway A, Grundheber A, Stender E, Willershausen B. Comparison of the efficacy of chemomechanical caries removal (Carisolv) with that of conventional excavation in reducing the cariogenic flora. Int J Paediatr Dent. 2004;14(3):182–91. Pandit I, Srivastava N, Gugnani N, Gupta M VL. Various methods of caries removal in children: A comparative clinical study. J Ind Soc Pedod Prev Dent. 2007;25(2):93–6. Subramaniam P, Babu K, Neeraja G. Comparison of the antimicrobial efficacy of chemomechanical caries removal (Carisolv) with that of conventional drilling in reducing cariogenic flora. J Clin Pediatr Dent. 2008;32(3):215–9. Kochhar GK, Srivastava N, Pandit IK, Gugnani N GM. An evaluation of different caries removal techniques in primary teeth: a comparitive clinical study. J Clin Pediatr Dent. 2011;36(1):5–9. Kirzioglu Z, Gurbuz T, Yilmaz Y. Clinical evaluation of chemomechanical and mechanical caries removal: status of the restorations at 3, 6, 9 and 12 months. Clin Oral Investig. 2007 Mar;11(1):69–76. Nadanovsky P, Cohen Carneiro F, Souza de Mello F. Removal of caries using only hand instruments: a comparison of mechanical and chemo-mechanical methods. Caries Res. 2001;35(5):384–9. Maru VP, Kumar A, Badiyani BK, Sharma AR, Sharma J, Dobariya CV. Behavioral changes in preschoolers treated with/without rotary instruments. J Int Soc Prev Community Dent. 2014 May;4(2):77–81. Schwendicke F, Frencken J, Bjřrndal L, Maltz M, Manton D, Ricketts D, et al. Managing Carious Lesions: Consensus Recommendations on Carious Tissue Removal. Adv Dent Res. 2016;28(2):58–67. NCT01641861. A Comparative study of Papacarie and the Conventional Method for dental caries treatment. | Link |





 Research papers
Research papersSystematization of initiatives in sexual and reproductive health about good practices criteria in response to the COVID-19 pandemic in primary health care in Chile
Clinical, psychological, social, and family characterization of suicidal behavior in Chilean adolescents: a multiple correspondence analysis
