
Key Words: Rhegmatogenous retinal detachment, pseudophakic, aphakic, pars plana vitrectomy, scleral buckle, Epistemonikos, GRADE.
Abstract
INTRODUCTION
Cataract surgery increases the risk for rhegmatogenous retinal detachment. Pars plana vitrectomy and scleral buckling are two surgical procedures used for its repair. The combination of both techniques had been proposed for rhegmatogenous retinal detachment in patients with previous cataract surgery (pseudophakic or aphakic), but its effectiveness remains unclear.
METHODS
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS
We identified four systematic reviews with eight studies overall, one of them was a randomized trial. With this data, we conclud-ed that pars plana vitrectomy plus scleral buckle may make little or no difference in primary or final retinal reattachment rate nor in final visual acuity, but the certainty of the evidence is low. In terms of surgery complications, we are uncertain if vitrecto-my plus scleral buckle increases the risk of proliferative vitreoretinopathy or reduces the risk of glaucoma because the certainty of the evidence is very low.
Problem
Rhegmatogenous retinal detachment is defined as the separation of the neurosensory retina from the underlying retinal pigment epithelium. Cataract surgery, an intervention that aims to replace the natural lens by an artificial lens (pseudophakia), could increase the risk of retinal detachment by a factor of seven to eight times [1], [2].
Pars plana vitrectomy and scleral buckle (or encircling band) are two surgical procedures employed to repair retinal detachments. Pars plana vitrectomy consists in the removal of vitreous gel associated with laser and injection of gas or silicone oil to compress the retina. In scleral buckle, the surgeon sutures a silicone implant to the outer surface of the sclera creating an indentation in the wall of the eye to achieve the apposition of the neurosensory retina and retinal pigment epithelium. Finally, the retinal break is repaired with cryotherapy or laser.
Although there is evidence about the effectiveness of these techniques separately in pseudophakic retinal detachments [3], it is not clear whether the combination of scleral buckling with pars plana vitrectomy is superior in patients with an artificial lens (pseudophakic) or patients without an intraocular lens (aphakic).
Methods
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We identified four systematic reviews [4], [5], [6], [7] including eight primary studies [8],[9],[10],[11],[12],[13],[14],[15], one of which is a randomized control trial [9]. We excluded four studies from the analysis: in three of them [12], [13], [14] the comparison was unclear according to the information provided by the systematic reviews. In one study [15], the population had an additional condition besides retinal detachment. This table and the summary are based on the randomized trial [9] because the observational studies did not increase the certainty of the evidence nor provided additional relevant information. |
|
What types of patients were included* |
All patients included in the randomized trial [9] were pseudophakic with rhegmatogenous retinal detachment and inferior retinal tear. The mean age was 57 years old for the pars plana vitrectomy group and 61 years for the pars plana vitrectomy plus scleral buckle group. Patients had macular detachment (73% of the patients in pars plana vitrectomy group and 63% of the patients in pars plana vitrectomy plus scleral buckle group) and proliferative vitreoretinopathy at grade C or worse (27% of the patients from the pars plana vitrectomy group and 3% of the patients with pars plana vitrectomy plus scleral buckle group). |
|
What types of interventions were included* |
The trial [9] compared pars plana vitrectomy plus scleral buckle with pars plana vitrectomy alone. Laser photocoagulation in 360° and silicone oil instillation were performed in all patients randomized to the pars plana vitrectomy group. The scleral buckle was conducted using a 360° encircling band in the group which received both procedures. The systematic review [6] did not describe the procedure used to perform pars plana vitrectomy and scleral buckle. Neither if laser photocoagulation in 360° was applied nor if instillation of air or gas was used in the pars plana vitrectomy plus scleral buckle group. |
|
What types of outcomes |
The systematic review [6] evaluated multiple outcomes, which were grouped as follows:
|
* Information about primary studies is not extracted directly from primary studies but from identified systematic reviews, unless otherwise stated.
Summary of findings
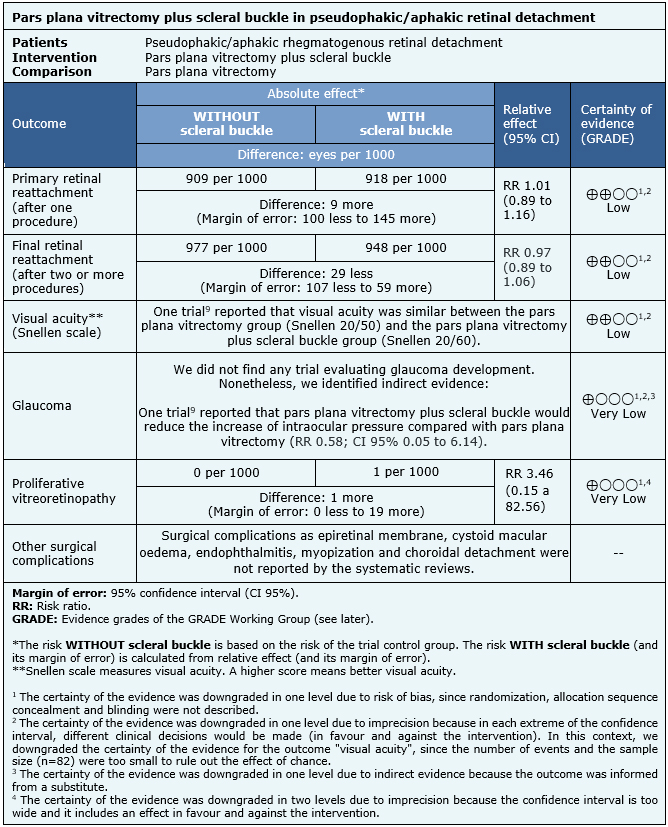
The information about the outcomes of pars plana vitrectomy plus scleral buckle compared with pars plana vitrectomy in pseudophakic retinal detachment is based in one randomized controlled trial [9] which included 82 pseudophakic eyes.
The trial measured the following outcomes: primary retinal reattachment (retinal reattachment after one procedure) (82 eyes), final retinal reattachment (retinal reattachment after two or more procedures) (82 eyes) and visual acuity in Snellen scale (82 eyes). The latter is reported as a narrative synthesis since none of the systematic reviews provided the necessary information to perform a meta-analysis.
The trial [9] reported complications as proliferative vitreoretinopathy and increased ocular pressure (indirect evidence for the development of glaucoma) (82 eyes). Other surgical complications as epiretinal membrane, cystoid macular oedema, endophthalmitis, myopization and choroidal detachment were not described by the systematic reviews.
The summary of findings is as follows:
- Pars plana vitrectomy plus scleral buckle compared with pars plana vitrectomy may make little or no difference in primary retinal reattachment (low certainty evidence).
- Pars plana vitrectomy plus scleral buckle compared with pars plana vitrectomy may slightly increase final retinal reattachment rate (low certainty evidence).
- Pars plana vitrectomy plus scleral buckle compared with pars plana vitrectomy may make little or no difference to visual acuity (low certainty evidence).
- We are uncertain whether pars plana vitrectomy plus scleral buckle compared with pars plana vitrectomy reduces the risk of glaucoma because the certainty of the evidence has been assessed as very low.
- We are uncertain whether pars plana vitrectomy plus scleral buckle compared with pars plana vitrectomy reduces the risk of proliferative vitreoretinopathy because the certainty of the evidence has been assessed as very low.
- The outcome “other complications of the surgery” was not reported by the evidence included in this article.
| Follow the link to access the interactive version of this table (Interactive Summary of Findings – iSoF) |

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
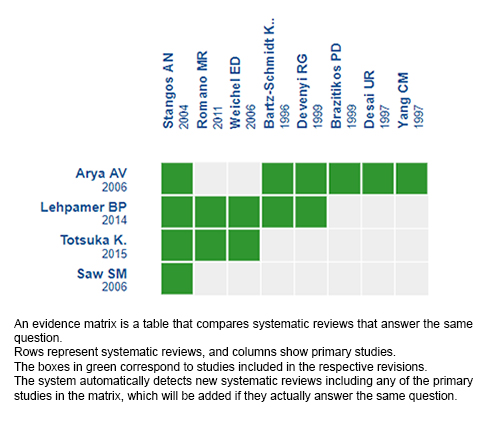
Follow the link to access the interactive version: Pars plana vitrectomy plus scleral buckle versus pars plana vitrectomy in pseudophakic/aphakic retinal detachment.
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
 Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.

INTRODUCCIÓN
La cirugía de cataratas es un factor de riesgo para el desprendimiento de retina regmatógeno. Dentro de las técnicas utilizadas para su reparación, se encuentran la vitrectomía pars plana y la banda de silicona. La combinación de ambas técnicas ha sido propuesta en pacientes con desprendimiento de retina previamente operados de cataratas (pseudofáquicos o afáquicos), pero su efectividad no está clara.
MÉTODOS
Realizamos una búsqueda en Epistemonikos, la mayor base de datos de revisiones sistemáticas en salud, la cual es mantenida mediante el cribado de múltiples fuentes de información, incluyendo MEDLINE, EMBASE, Cochrane, entre otras. Extrajimos los datos desde las revisiones identificadas, analizamos los datos de los estudios primarios, realizamos un metanálisis y preparamos una tabla de resumen de los resultados utilizando el método GRADE.
RESULTADOS Y CONCLUSIONES
Identificamos cuatro revisiones sistemáticas que en conjunto incluyeron ocho estudios primarios, de los cuales, uno corresponde a un ensayo aleatorizado. A partir de éste, concluimos que la combinación de vitrectomía pars plana y banda de silicona podría resultar en poca o nula diferencia en la reaplicación retinal primaria, en la reaplicación retinal final y en la agudeza visual, pero la certeza de la evidencia es baja. Respecto a las complicaciones, no es posible establecer con claridad si la combinación de ambas técnicas aumenta la frecuencia de vitreorretinopatía proliferativa o si disminuye el desarrollo de glaucoma, debido a que la certeza de la evidencia fue evaluada como muy baja.
Authors:
Ana Sanhueza[1,2], Raúl González[2,3]
Affiliation:
[1] Facultad de Medicina, Pontificia Universidad Católica de Chile, Santiago, Chile.
[2] Proyecto Epistemonikos, Santiago, Chile.
[3] Departamento de Oftalmología, Facultad de Medicina, Pontificia Universidad Católica de Chile, Santiago, Chile.
E-mail: raulgonzalezc@gmail.com
Author address:
[1] Centro Evidencia UC Pontificia Universidad Católica de Chile Diagonal Paraguay 476 Santiago Chile
Citation: Sanhueza A, González R. Pars plana vitrectomy plus scleral buckle versus pars plana vitrec-tomy in pseudophakic retinal detachment. Medwave 2020;20(06):e7964 doi: 10.5867/medwave.2020.06.7964
Submission date: 5/12/2019
Acceptance date: 12/12/2019
Publication date: 22/7/2020
Origin: This article is a product of the Evidence Synthesis Project of Epistemonikos Fundation, in collaboration with Medwave for its publication.
Type of review: Not non-blind peers by the UC Evidence Center methodological team in collaboration with Epistemonikos Evidence Synthesis Project.
Comments (0)
We are pleased to have your comment on one of our articles. Your comment will be published as soon as it is posted. However, Medwave reserves the right to remove it later if the editors consider your comment to be: offensive in some sense, irrelevant, trivial, contains grammatical mistakes, contains political harangues, appears to be advertising, contains data from a particular person or suggests the need for changes in practice in terms of diagnostic, preventive or therapeutic interventions, if that evidence has not previously been published in a peer-reviewed journal.
No comments on this article.
To comment please log in
Medwave provides HTML and PDF download counts as well as other harvested interaction metrics. There may be a 48-hour delay for most recent metrics to be posted.
- Boberg-Ans G, Henning V, Villumsen J, la Cour M. Longterm incidence of rhegmatogenous retinal detachment and survival in a defined population undergoing standardized phacoemulsification surgery. Acta Acta Ophthalmol Scand. 2006 Oct;84(5):613-8. | CrossRef | PubMed |
- Norregaard JC, Thoning H, Andersen TF, Bernth-Petersen P, Javitt JC, Anderson GF. Risk of retinal detachment following cataract extraction: results from the International Cataract Surgery Outcomes Study. Br J Ophthalmol. 1996 Aug;80(8):689-93. | CrossRef | PubMed | PMC |
- Znaor L, Medic A, Binder S, Vucinovic A, Marin Lovric J, Puljak L. Pars plana vitrectomy versus scleral buckling for repairing simple rhegmatogenous retinal detachments. Cochrane Database Syst Rev. 2019 Mar 8;3:CD009562. | CrossRef | PubMed | PMC |
- Arya AV, Emerson JW, Engelbert M, Hagedorn CL, Adelman RA. Surgical management of pseudophakic retinal detachments: a meta-analysis. Ophthalmology. 2006 Oct;113(10):1724-33. | CrossRef | PubMed |
- Saw SM, Gazzard G, Wagle AM, Lim J, Au Eong KG. An evidence-based analysis of surgical interventions for uncomplicated rhegmatogenous retinal detachment. Acta Ophthalmol Scand. 2006 Oct;84(5):606-12. | CrossRef | PubMed |
- Totsuka K, Inui H, Roggia MF, Hirasawa K, Noda Y, Ueta T. Supplemental scleral buckle in vitrectomy for the repair of rhegmatogenous retinal detachment: A Systematic Review of Literature and Meta-Analysis. Retina. 2015 Nov;35(11):2423-31. | CrossRef | PubMed |
- Lehpamer BP, Carvounis PE. Vitrectomy with and without scleral buckling for retinal detachment repair in pseudophakic patients. Int Ophthalmol Clin. 2014 Spring;54(2):79-90. | CrossRef | PubMed |
- Stangos AN, Petropoulos IK, Brozou CG, Kapetanios AD, Whatham A, Pournaras CJ. Pars-plana vitrectomy alone vs vitrectomy with scleral buckling for primary rhegmatogenous pseudophakic retinal detachment. Am J Ophthalmol. 2004 Dec;138(6):952-8. | CrossRef | PubMed |
- Romano MR, Angi M, Valldeperas X, Costagliola C, Vinciguerra P. Twenty-three-gauge pars plana vitrectomy, Densiron-68, and 360° endolaser versus combined 20-gauge pars plana vitrectomy, scleral buckle, and SF6 for pseudophakic retinal detachment with inferior retinal breaks. Retina. 2011 Apr;31(4):686-91. | CrossRef | PubMed |
- Brazitikos PD, D'Amico DJ, Tsinopoulos IT, Stangos NT. Primary vitrectomy with perfluoro-n-octane use in the treatment of pseudophakic retinal detachment with undetected retinal breaks. Retina. 1999;19(2):103-9. | PubMed |
- Weichel ED, Martidis A, Fineman MS, McNamara JA, Park CH, Vander JF, Ho AC, Brown GC. Pars plana vitrectomy versus combined pars plana vitrectomy-scleral buckle for primary repair of pseudophakic retinal detachment. Ophthalmology. 2006 Nov;113(11):2033-40. | CrossRef | PubMed |
- Desai UR, Strassman IB. Combined pars plana vitrectomy and scleral buckling for pseudophakic and aphakic retinal detachments in which a break is not seen preoperatively. Ophthalmic Surg Lasers. 1997 Sep;28(9):718-22. | CrossRef | PubMed |
- Devenyi RG, de Carvalho Nakamura H. Combined scleral buckle and pars plana vitrectomy as a primary procedure for pseudophakic retinal detachments. Ophthalmic Surg Lasers. 1999 Sep-Oct;30(8):615-8. | CrossRef | PubMed |
- Bartz-Schmidt KU, Kirchhof B, Heimann K. Primary vitrectomy for pseudophakic retinal detachment. Br J Ophthalmol. 1996 Apr;80(4):346-9. | CrossRef | PubMed |
- Yang CM. Pars plana vitrectomy in the treatment of combined rhegmatogenous retinal detachment and choroidal detachment in aphakic or pseudophakic patients. Ophthalmic Surg Lasers. 1997 Apr;28(4):288-93. | PubMed |
- Walter P, Hellmich M, Baumgarten S, Schiller P, Limburg E, Agostini H, Pielen A, Helbig H, Lommatzsch A, Rössler G, Mazinani B; VIPER Study Group. Vitrectomy with and without encircling band for pseudophakic retinal detachment: VIPER Study Report No 2-main results. Br J Ophthalmol. 2017 Jun;101(6):712-718. | CrossRef | PubMed |
Boberg-Ans G, Henning V, Villumsen J, la Cour M. Longterm incidence of rhegmatogenous retinal detachment and survival in a defined population undergoing standardized phacoemulsification surgery. Acta Acta Ophthalmol Scand. 2006 Oct;84(5):613-8. | CrossRef | PubMed |Norregaard JC, Thoning H, Andersen TF, Bernth-Petersen P, Javitt JC, Anderson GF. Risk of retinal detachment following cataract extraction: results from the International Cataract Surgery Outcomes Study. Br J Ophthalmol. 1996 Aug;80(8):689-93. | CrossRef | PubMed | PMC |Znaor L, Medic A, Binder S, Vucinovic A, Marin Lovric J, Puljak L. Pars plana vitrectomy versus scleral buckling for repairing simple rhegmatogenous retinal detachments. Cochrane Database Syst Rev. 2019 Mar 8;3:CD009562. | CrossRef | PubMed | PMC |Arya AV, Emerson JW, Engelbert M, Hagedorn CL, Adelman RA. Surgical management of pseudophakic retinal detachments: a meta-analysis. Ophthalmology. 2006 Oct;113(10):1724-33. | CrossRef | PubMed |Saw SM, Gazzard G, Wagle AM, Lim J, Au Eong KG. An evidence-based analysis of surgical interventions for uncomplicated rhegmatogenous retinal detachment. Acta Ophthalmol Scand. 2006 Oct;84(5):606-12. | CrossRef | PubMed |Totsuka K, Inui H, Roggia MF, Hirasawa K, Noda Y, Ueta T. Supplemental scleral buckle in vitrectomy for the repair of rhegmatogenous retinal detachment: A Systematic Review of Literature and Meta-Analysis. Retina. 2015 Nov;35(11):2423-31. | CrossRef | PubMed |Lehpamer BP, Carvounis PE. Vitrectomy with and without scleral buckling for retinal detachment repair in pseudophakic patients. Int Ophthalmol Clin. 2014 Spring;54(2):79-90. | CrossRef | PubMed |Stangos AN, Petropoulos IK, Brozou CG, Kapetanios AD, Whatham A, Pournaras CJ. Pars-plana vitrectomy alone vs vitrectomy with scleral buckling for primary rhegmatogenous pseudophakic retinal detachment. Am J Ophthalmol. 2004 Dec;138(6):952-8. | CrossRef | PubMed |Romano MR, Angi M, Valldeperas X, Costagliola C, Vinciguerra P. Twenty-three-gauge pars plana vitrectomy, Densiron-68, and 360° endolaser versus combined 20-gauge pars plana vitrectomy, scleral buckle, and SF6 for pseudophakic retinal detachment with inferior retinal breaks. Retina. 2011 Apr;31(4):686-91. | CrossRef | PubMed |Brazitikos PD, D'Amico DJ, Tsinopoulos IT, Stangos NT. Primary vitrectomy with perfluoro-n-octane use in the treatment of pseudophakic retinal detachment with undetected retinal breaks. Retina. 1999;19(2):103-9. | PubMed |Weichel ED, Martidis A, Fineman MS, McNamara JA, Park CH, Vander JF, Ho AC, Brown GC. Pars plana vitrectomy versus combined pars plana vitrectomy-scleral buckle for primary repair of pseudophakic retinal detachment. Ophthalmology. 2006 Nov;113(11):2033-40. | CrossRef | PubMed |Desai UR, Strassman IB. Combined pars plana vitrectomy and scleral buckling for pseudophakic and aphakic retinal detachments in which a break is not seen preoperatively. Ophthalmic Surg Lasers. 1997 Sep;28(9):718-22. | CrossRef | PubMed |Devenyi RG, de Carvalho Nakamura H. Combined scleral buckle and pars plana vitrectomy as a primary procedure for pseudophakic retinal detachments. Ophthalmic Surg Lasers. 1999 Sep-Oct;30(8):615-8. | CrossRef | PubMed |Bartz-Schmidt KU, Kirchhof B, Heimann K. Primary vitrectomy for pseudophakic retinal detachment. Br J Ophthalmol. 1996 Apr;80(4):346-9. | CrossRef | PubMed |Yang CM. Pars plana vitrectomy in the treatment of combined rhegmatogenous retinal detachment and choroidal detachment in aphakic or pseudophakic patients. Ophthalmic Surg Lasers. 1997 Apr;28(4):288-93. | PubMed |Walter P, Hellmich M, Baumgarten S, Schiller P, Limburg E, Agostini H, Pielen A, Helbig H, Lommatzsch A, Rössler G, Mazinani B; VIPER Study Group. Vitrectomy with and without encircling band for pseudophakic retinal detachment: VIPER Study Report No 2-main results. Br J Ophthalmol. 2017 Jun;101(6):712-718. | CrossRef | PubMed |





 Research papers
Research papersSystematization of initiatives in sexual and reproductive health about good practices criteria in response to the COVID-19 pandemic in primary health care in Chile
Clinical, psychological, social, and family characterization of suicidal behavior in Chilean adolescents: a multiple correspondence analysis
