
Abstract
INTRODUCTION
Cachexia and anorexia are among the most frequent symptoms in patients with cancer. Cannabinoids have been used in patients with advanced cancer; however, their role is still controversial.
METHODS
To answer this question we used Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS
We identified ten systematic reviews including three studies overall, of which two were randomized trials. We concluded it is not clear whether cannabinoids have any positive effect on increasing weight because the certainty of the evidence is very low. They might not have any effect on appetite, and are probably associated to frequent adverse effects.
Problem
The anorexia-cachexia syndrome corresponds to an hypercatabolic state characterized by an absence of desire to eat and an involuntary weight loss associated with a loss of muscle mass. This phenomenon is observed in up to 80% of patients with cancer and in variable percentages in patients with other non-oncological diseases [1].
In oncological patients, anorexia is explained by a variety of causes (e.g. dysphagia, dry mouth, nausea, depression), which determine a decrease in intake and in the availability of nutrients, and as a consequence, weight loss. In patients with isolated anorexia, the increase of the intake and the availability of nutrients can revert weight loss. Although anorexia by itself does not explain the deterioration observed in cancer patients, it is a factor that contributes to weight loss and is considered a relevant parameter in the quality of life [2]. Cachexia corresponds to a multifactorial syndrome characterized by loss of skeletal muscle mass, with or without loss of fat mass, which leads to progressive functional deterioration [3]. It is among the most common symptoms in cancer patients, with a prevalence of 50% at the time of diagnosis and 80% at the end-of-life stage. It is associated with a decrease in quality of life and survival (it can be the direct cause of 20% of deaths related to this disease) and to other symptoms such as anorexia (in up to 90% of cancer patients), fatigue, asthenia, weakness, early satiety, among others [4]. It is known the pathophysiology of cachexia is multifactorial; for example, tumor growth is associated with profound metabolic and neurochemical alterations, such as the production of a series of proinflammatory cytokines, including TNF-alpha, IL-1 and IL-6, which favour an hypercatabolic state and hamper the use of available nutrients.
Several interventions focused on these particular mechanisms have been proposed, within which we find progestogens, corticoids and cannabinoids [5], the latter would seek to improve appetite through the activation of the CB 1 (central nervous system) and CB 2 (immune cells) receptors of the endocannabidiol system [6], and to decrease weight loss through immunomodulating effect of cytokines [7]. However, it is not clear if this theory actually translates into a clinical effect.
Methods
To answer the question, we used Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We found 10 systematic reviews [8],[9],[10],[11],[12],[13],[14],[15],[16],[17] that included three primary studies relevant to the question [18],[19],[20]; two of these correspond to randomized trials [18],[19]. This table and the summary in general are based on the latter. |
|
What types of patients were included* |
Both trials included adults (older than 18 years), of both sexes with solid or stage IV hematologic cancer. One trial established inclusion criteria for weight loss in the last 2 to 6 months and also selected by ECOG less than 2 [18]. |
|
What types of interventions were included* |
Both trials evaluated oral delta-9-tetrahydrocannabinol (THC). One trial [18] used oral THC (5 mg / day) and cannabidiol (2 mg / day) for six weeks versus placebo. The other trial [19] used only oral THC in three daily doses (0.1 mg / kg / day) for two weeks versus placebo. |
|
What types of outcomes |
The trials measured multiple outcomes, but the systematic reviews pooled them as follows:
|
* The information about primary studies is extracted from the systematic reviews identified, unless otherwise specified.
Summary of Findings
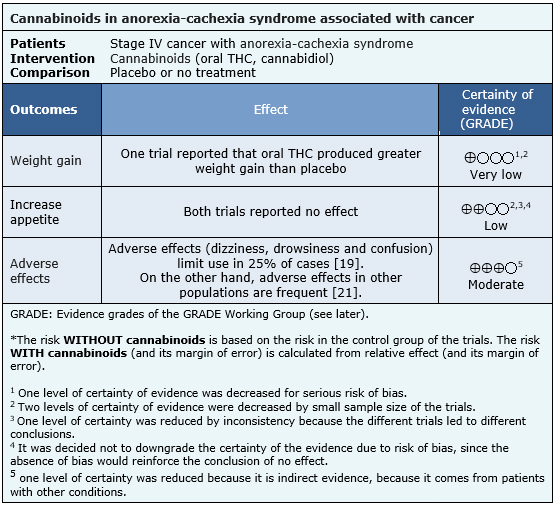
The information about the effects of cannabinoids for anorexia-cachexia syndrome in patients with advanced cancer is based on two randomized trials involving 218 patients.
One trial [18] reported weight gain (164 patients). Both trials [18],[19] reported increased appetite (218 patients).
The summary of findings is as follows:
- It is not clear whether the use of cannabinoids leads to weight gain in patients with advanced cancer, because the certainty of the evidence is very low.
- The use of cannabinoids might not increase appetite in patients with advanced cancer. The certainty of the evidence is low.
- The use of cannabinoids is probably associated to frequent adverse effects. The certainty of the evidence is moderate.

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
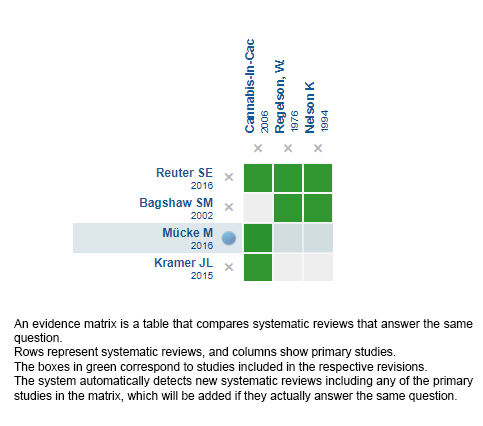
Follow the link to access the interactive version: Cannabinoids versus placebo for cachexia-anorexia syndrome
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
 Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.

INTRODUCCIÓN
La caquexia y la anorexia se encuentran dentro de los síntomas más frecuentes en los pacientes oncológicos. Los cannabinoides han sido propuestos para su manejo en los pacientes con cáncer avanzado, sin embargo, su rol es controvertido.
MÉTODOS
Para responder esta pregunta utilizamos Epistemonikos, la mayor base de datos de revisiones sistemáticas en salud a nivel mundial, la cual es mantenida mediante búsquedas en múltiples fuentes de información, incluyendo MEDLINE, EMBASE, Cochrane, entre otras. Extrajimos los datos desde las revisiones identificadas, reanalizamos los datos de los estudios primarios y preparamos una tabla de resumen de los resultados utilizando el método GRADE.
RESULTADOS Y CONCLUSIONES
Identificamos diez revisiones sistemáticas, que en conjunto incluyen tres estudios, entre ellos dos ensayos aleatorizados. Concluimos que no está claro si los cannabinoides logran o no un aumento de peso en pacientes con anorexia-caquexia porque la certeza de la evidencia es muy baja, podrían no tener tampoco efecto sobre el apetito, y probablemente se asocian a efectos adversos frecuentes.
Authors:
Claudia Cabeza[1,3], Oscar Corsi[2,3], Pedro Pérez-Cruz[2,3,4]
Affiliation:
[1] Facultad de Medicina, Pontificia Universidad Católica de Chile, Santiago, Chile
[2] Departamento de Medicina Interna, Facultad de Medicina, Pontificia Universidad Católica de Chile, Santiago, Chile
[3] Proyecto Epistemonikos, Santiago, Chile
[4] Programa de Medicina Paliativa y Cuidados Continuos, Facultad de Medicina, Pontificia Universidad Católica de Chile, Santiago, Chile
E-mail: pperezc@med.puc.cl
Author address:
[1] Centro Evidencia UC Pontificia Universidad Católica de Chile Centro de Innovación UC Anacleto Angelini Avda.Vicuńa Mackenna 4860 Macul Santiago Chile
Citation: Cabeza C, Corsi O, Pérez-Cruz PE. Are cannabinoids an alternative for cachexia-anorexia syndrome in patients with advanced cancer?. Medwave 2017 Nov-Dic;17(9):e7130 doi: 10.5867/medwave.2017.09.7130
Submission date: 17/11/2017
Acceptance date: 20/12/2017
Publication date: 29/12/2017
Origin: This article is a product of the Evidence Synthesis Project of Epistemonikos Fundation, in collaboration with Medwave for its publication.
Type of review: Non-blinded peer review by members of the methodological team of Epistemonikos Evidence Synthesis Project.
Comments (0)
We are pleased to have your comment on one of our articles. Your comment will be published as soon as it is posted. However, Medwave reserves the right to remove it later if the editors consider your comment to be: offensive in some sense, irrelevant, trivial, contains grammatical mistakes, contains political harangues, appears to be advertising, contains data from a particular person or suggests the need for changes in practice in terms of diagnostic, preventive or therapeutic interventions, if that evidence has not previously been published in a peer-reviewed journal.
No comments on this article.
To comment please log in
Medwave provides HTML and PDF download counts as well as other harvested interaction metrics. There may be a 48-hour delay for most recent metrics to be posted.
- Del Fabbro E, Dalal S, Bruera E. Symptom control in palliative care--Part II: cachexia/anorexia and fatigue. J Palliat Med. 2006 Apr;9(2):409-21. | PubMed |
- Bruera E. ABC of palliative care. Anorexia, cachexia, and nutrition. BMJ. 1997 Nov 8;315(7117):1219-22 | PubMed | PMC |
- Fearon K, Strasser F, Anker SD, Bosaeus I, Bruera E, Fainsinger RL, Jatoi A, Loprinzi C, MacDonald N, Mantovani G, Davis M, Muscaritoli M, Ottery F, Radbruch L, Ravasco P, Walsh D, Wilcock A, Kaasa S, Baracos VE. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol. 2011 May;12(5):489-95. | CrossRef | PubMed |
- Laviano A, Meguid MM, Inui A, Muscaritoli M, Rossi-Fanelli F. Therapy insight: Cancer anorexia-cachexia syndrome--when all you can eat is yourself. Nat Clin Pract Oncol. 2005 Mar;2(3):158-65. | PubMed |
- Aapro M, Arends J, Bozzetti F, Fearon K, Grunberg SM, Herrstedt J, Hopkinson J, Jacquelin-Ravel N, Jatoi A, Kaasa S, Strasser F; ESMO (European School of Medical Oncology).. Early recognition of malnutrition and cachexia in the cancer patient: a position paper of a European School of Oncology Task Force. Ann Oncol. 2014 Aug;25(8):1492-9. | CrossRef | PubMed |
- Mechoulam R, Parker LA. The endocannabinoid system and the brain. Annu Rev Psychol. 2013;64:21-47. | CrossRef | PubMed |
- Massa F, Marsicano G, Hermann H, Cannich A, Monory K, Cravatt BF, Ferri GL, Sibaev A, Storr M, Lutz B. The endogenous cannabinoid system protects against colonic inflammation. J Clin Invest. 2004 Apr;113(8):1202-9. | PubMed | PMC |
- Amato L, Davoli M, Minozzi S, Mitrova Z, Parmelli E, Saulle R, Vecchi S. Systematic reviews on therapeutic efficacy and safety of Cannabis (including extracts and tinctures) for patients with multiple sclerosis, chronic neuropathic pain, dementia and Tourette syndrome, HIV/AIDS, and cancer receiving chemotherapy. Departament of Epidemiology Lazio Regional Healty Service. 2016.
- Bagshaw SM, Hagen NA. Medical efficacy of cannabinoids and marijuana: a comprehensive review of the literature. Journal of palliative care. 2002;18(2):111-22.
- Ben Amar M. Cannabinoids in medicine: A review of their therapeutic potential. J Ethnopharmacol. 2006 Apr 21;105(1-2):1-25. | PubMed |
- Goldenberg M, Reid MW, IsHak WW, Danovitch I. The impact of cannabis and cannabinoids for medical conditions on health-related quality of life: A systematic review and meta-analysis. Drug Alcohol Depend. 2017 May 1;174:80-90. | CrossRef | PubMed |
- Hazekamp A, Grotenhermen F. Review on clinical studies with cannabis and cannabinoids 2005–2009. Cannabinoids. 2010 Feb 13; 5(special): 1–21. | Link |
- Kairuz MJF. Systematic review of clinical studies on cannabis use for therapeutic purposes between 2005-2015. 2015.
- Kramer JL. Medical marijuana for cancer. CA Cancer J Clin. 2015 Mar;65(2):109-22. | CrossRef | PubMed |
- Mücke M, Carter C, Cuhls H, Prüß M, Radbruch L, Häuser W. [Cannabinoids in palliative care: Systematic review and meta-analysis of efficacy, tolerability and safety]. Schmerz. 2016 Feb;30(1):25-36. | CrossRef | PubMed |
- Reuter SE, Martin JH. Pharmacokinetics of Cannabis in Cancer Cachexia-Anorexia Syndrome. Clin Pharmacokinet. 2016 Jul;55(7):807-12. | CrossRef | PubMed |
- Zhornitsky S, Potvin S. Cannabidiol in humans-the quest for therapeutic targets. Pharmaceuticals (Basel). 2012 May 21;5(5):529-52. | CrossRef | PubMed | PMC |
- Cannabis-In-Cachexia-Study-Group., Strasser F, Luftner D, Possinger K, Ernst G, Ruhstaller T, Meissner W, Ko YD, Schnelle M, Reif M, Cerny T. Comparison of orally administered cannabis extract and delta-9-tetrahydrocannabinol in treating patients with cancer-related anorexia-cachexia syndrome: a multicenter, phase III, randomized, double-blind, placebo-controlled clinical trial from the Cannabis-In-Cachexia-Study-Group. J Clin Oncol. 2006 Jul 20;24(21):3394-400. | PubMed |
- Regelson W, Butler JR, Schulz J, Kirk T, Peek L, Green ML, Zalis MO. Delta-9-tetrahydrocannabinol as an effective antidepressant and appetite-stimulating agent in advanced cancer patients. In: Braude MC, Szara S. (Eds.). The Pharmacology of Marihuana. 1976. Raven Press, New York. pp. 763–776.
- Nelson K, Walsh D, Deeter P, Sheehan F. A phase II study of delta-9-tetrahydrocannabinol for appetite stimulation in cancer-associated anorexia. J Palliat Care. 1994 Spring;10(1):14-8. | PubMed |
- Whiting PF, Wolff RF, Deshpande S, Di Nisio M, Duffy S, Hernandez AV, Keurentjes JC, Lang S, et al. Cannabinoids for Medical Use: A Systematic Review and Meta-analysis. JAMA. 2015 Jun 23-30;313 (24):2456-73.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Palliative Care 1.2017 [cited May 18, 2017] | Link |
Del Fabbro E, Dalal S, Bruera E. Symptom control in palliative care--Part II: cachexia/anorexia and fatigue. J Palliat Med. 2006 Apr;9(2):409-21. | PubMed |Bruera E. ABC of palliative care. Anorexia, cachexia, and nutrition. BMJ. 1997 Nov 8;315(7117):1219-22 | PubMed | PMC |Fearon K, Strasser F, Anker SD, Bosaeus I, Bruera E, Fainsinger RL, Jatoi A, Loprinzi C, MacDonald N, Mantovani G, Davis M, Muscaritoli M, Ottery F, Radbruch L, Ravasco P, Walsh D, Wilcock A, Kaasa S, Baracos VE. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol. 2011 May;12(5):489-95. | CrossRef | PubMed |Laviano A, Meguid MM, Inui A, Muscaritoli M, Rossi-Fanelli F. Therapy insight: Cancer anorexia-cachexia syndrome--when all you can eat is yourself. Nat Clin Pract Oncol. 2005 Mar;2(3):158-65. | PubMed |Aapro M, Arends J, Bozzetti F, Fearon K, Grunberg SM, Herrstedt J, Hopkinson J, Jacquelin-Ravel N, Jatoi A, Kaasa S, Strasser F; ESMO (European School of Medical Oncology).. Early recognition of malnutrition and cachexia in the cancer patient: a position paper of a European School of Oncology Task Force. Ann Oncol. 2014 Aug;25(8):1492-9. | CrossRef | PubMed |Mechoulam R, Parker LA. The endocannabinoid system and the brain. Annu Rev Psychol. 2013;64:21-47. | CrossRef | PubMed |Massa F, Marsicano G, Hermann H, Cannich A, Monory K, Cravatt BF, Ferri GL, Sibaev A, Storr M, Lutz B. The endogenous cannabinoid system protects against colonic inflammation. J Clin Invest. 2004 Apr;113(8):1202-9. | PubMed | PMC |Amato L, Davoli M, Minozzi S, Mitrova Z, Parmelli E, Saulle R, Vecchi S. Systematic reviews on therapeutic efficacy and safety of Cannabis (including extracts and tinctures) for patients with multiple sclerosis, chronic neuropathic pain, dementia and Tourette syndrome, HIV/AIDS, and cancer receiving chemotherapy. Departament of Epidemiology Lazio Regional Healty Service. 2016. Bagshaw SM, Hagen NA. Medical efficacy of cannabinoids and marijuana: a comprehensive review of the literature. Journal of palliative care. 2002;18(2):111-22. Ben Amar M. Cannabinoids in medicine: A review of their therapeutic potential. J Ethnopharmacol. 2006 Apr 21;105(1-2):1-25. | PubMed |Goldenberg M, Reid MW, IsHak WW, Danovitch I. The impact of cannabis and cannabinoids for medical conditions on health-related quality of life: A systematic review and meta-analysis. Drug Alcohol Depend. 2017 May 1;174:80-90. | CrossRef | PubMed |Hazekamp A, Grotenhermen F. Review on clinical studies with cannabis and cannabinoids 2005–2009. Cannabinoids. 2010 Feb 13; 5(special): 1–21. | Link |Kairuz MJF. Systematic review of clinical studies on cannabis use for therapeutic purposes between 2005-2015. 2015. Kramer JL. Medical marijuana for cancer. CA Cancer J Clin. 2015 Mar;65(2):109-22. | CrossRef | PubMed |Mücke M, Carter C, Cuhls H, Prüß M, Radbruch L, Häuser W. [Cannabinoids in palliative care: Systematic review and meta-analysis of efficacy, tolerability and safety]. Schmerz. 2016 Feb;30(1):25-36. | CrossRef | PubMed |Reuter SE, Martin JH. Pharmacokinetics of Cannabis in Cancer Cachexia-Anorexia Syndrome. Clin Pharmacokinet. 2016 Jul;55(7):807-12. | CrossRef | PubMed |Zhornitsky S, Potvin S. Cannabidiol in humans-the quest for therapeutic targets. Pharmaceuticals (Basel). 2012 May 21;5(5):529-52. | CrossRef | PubMed | PMC |Cannabis-In-Cachexia-Study-Group., Strasser F, Luftner D, Possinger K, Ernst G, Ruhstaller T, Meissner W, Ko YD, Schnelle M, Reif M, Cerny T. Comparison of orally administered cannabis extract and delta-9-tetrahydrocannabinol in treating patients with cancer-related anorexia-cachexia syndrome: a multicenter, phase III, randomized, double-blind, placebo-controlled clinical trial from the Cannabis-In-Cachexia-Study-Group. J Clin Oncol. 2006 Jul 20;24(21):3394-400. | PubMed |Regelson W, Butler JR, Schulz J, Kirk T, Peek L, Green ML, Zalis MO. Delta-9-tetrahydrocannabinol as an effective antidepressant and appetite-stimulating agent in advanced cancer patients. In: Braude MC, Szara S. (Eds.). The Pharmacology of Marihuana. 1976. Raven Press, New York. pp. 763–776. Nelson K, Walsh D, Deeter P, Sheehan F. A phase II study of delta-9-tetrahydrocannabinol for appetite stimulation in cancer-associated anorexia. J Palliat Care. 1994 Spring;10(1):14-8. | PubMed |Whiting PF, Wolff RF, Deshpande S, Di Nisio M, Duffy S, Hernandez AV, Keurentjes JC, Lang S, et al. Cannabinoids for Medical Use: A Systematic Review and Meta-analysis. JAMA. 2015 Jun 23-30;313 (24):2456-73. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Palliative Care 1.2017 [cited May 18, 2017] | Link |





 Research papers
Research papersSystematization of initiatives in sexual and reproductive health about good practices criteria in response to the COVID-19 pandemic in primary health care in Chile
Clinical, psychological, social, and family characterization of suicidal behavior in Chilean adolescents: a multiple correspondence analysis
