
Key Words: COVID-19, Transients and Migrants, Health planning, Health education, Mental health
Abstract
Introduction
International migration is a social determinant of health. The past decade has seen a large exodus of Venezuelans within Latin America, including Chile. In the past months, the world has been facing the SARS-CoV-2 coronavirus pandemic and its respiratory disease COVID-19.
Objective
To explore what factors are associated with feeling prepared to face the COVID-19 pandemic among the Venezuelan population residing in Chile.
Methods
Cross-sectional quantitative study with an opinion poll design. An online self-reported survey in Spanish and Creole was designed and piloted with experts and international migrants. It was disseminated to various international migrant groups through networks of migrant and pro-migrant organizations and the Chilean public health care network across the national territory. An effective sample size for analysis of 1690 participants was reached, of which 1008 (60%) were from Venezuela and included in this analysis. Feeling prepared to face the COVID-19 pandemic (yes/no) among Venezuelan migrants was described, as well as relevant variables like sex, level of education, length of stay, healthcare provision, anxiety or depression due to COVID-19, confinement, and evaluation of the quality of the information provided by the COVID-19 government.
Results
65% of the Venezuelan participants reported not feeling prepared for the pandemic. Compared to Venezuelan migrants who feel prepared to face the COVID-19 pandemic, migrants who reported not feeling prepared were in a higher proportion female, with secondary education level, had arrived in Chile in the past year, do not have a job but want to work, and belong to the public healthcare provision.
Discussion
Receiving good quality information on the pandemic and mental health symptoms are important factors associated with feeling prepared to face COVID-19 in Venezuelan migrants in Chile, suggesting that increased attention towards the physical and mental health of Venezuelan migrants in Chile and the region is needed.
Main messages
|
Introduction
International migration is part of a broad conceptual framework developed by the United Nations and related to human mobility[1]. The International Organization for Migration defines an international migrant as “any person who is outside a State of which he or she is a citizen or national,” either permanently or temporarily and regardless of their legal status[2]. Migration is a critical event in a person’s life course, during which multiple protective and risk factors for health and wellbeing interact in complex and dynamic ways[3]. Migration is a cross-sectional social determinant of health[4], as individual health may be influenced by migration-related factors before, during, and after the process of migration and the social context around it[5].
International migration can influence health outcomes through different mechanisms[5]. Experiencing health risks and human rights violations can negatively influence health, yet social capital and social protection can buffer negative experiences and prevent the appearance of adverse events during migration[5]. However, many groups of international migrants experience structural vulnerability during mobility because of limited access to health care with regards to needs, both in transit and upon arrival in the receiving country[6],[7]. This is especially frequent in irregular international migrants, refugees, and those migrants who live in poverty[8]. Vulnerability can be compounded in children and adolescents, women, ethnic minorities, sexual diversities, people with chronic conditions or infectious diseases, among other groups with greater exposure to processes of exclusion and social marginalization[9],[10],[11]. Additionally, international migrants may experience lower social protection coverage[12], precarious employment and unsafe working conditions[13], and overcrowding[14].
The COVID-19 pandemic may have exacerbated the different dimensions of vulnerability and marginalization that international migrants experience, depending on their particular circumstances, either because of the pre-existing factors described previously or factors directly related to the management of the pandemic, such as border closure[15] and xenophobic scapegoating[16]. In that sense, taking into account all dimensions of migration as a social determinant of health is paramount to a comprehensive analysis of the effects of the COVID-19 pandemic on migrant populations.
Chile has become a receiving country of international migrants, mostly migrants from other Latin American countries. According to the latest report of the National Statistics Institute and the Department of Immigration and Migration of the Ministry of the Interior and Public Security published in 2019, there were 1 492 522 international migrants in Chile, 7.7% of the national population[17]. Venezuelan migrants represent the first country of origin of international migrants residing in Chile, with an estimated 30.5% of the total migrant population. Globally, approximately 4.3 million Venezuelan migrants, refugees, and asylum-seekers were living outside of their country of origin as of September 2019, with outflows that have been heavily increasing since 2017. This represents one of the largest modern exoduses of international migrants from Latin America in the past century, impacting the region’s national health systems´ capacity and planning directly.
In accordance with national legislation and international recommendations, the Ministry of Health in Chile has been promoting access to health services to these populations progressively, as urged by the WHO (World Health Organization) at the 61st World Health Assembly, Resolution WHA61.17 of 2008 and PAHO (Pan American Health Organization) at the 55th Directing Council of the Organization. The most important breakthrough with regards to international migrants’ access to health in Chile is the Supreme Decree Nº67 of 2016, which allows irregular migrants without a formal income to access public health services under the same conditions as Chileans who do not receive an income. Regular migrants may choose between public and private health coverage in equal conditions with regards to the locals. Considering global processes of migratory flows relevant to Chile, in 2015, the Ministry of Health in Chile launched the Pilot Health Plan for International Migrants, which was implemented in 2016 and 2017. The Plan made way for the Health Policy for International Migrants launched in October 2017 and its upcoming Action Plan. These efforts by the Ministry of Health in Chile have catalyzed the gradual expansion of the rights of the migrant population in the public health care system.
As of July 20, 2020, 14 599 613 people were diagnosed with COVID-19 worldwide, and 607 746 lives were claimed, mostly in the United States, Brazil, and India[18]. On that same date, Chile was ranked number eight in the ranking of confirmed cases, totaling 330 930 people. The global health crisis and the Chilean crisis have hit international migrant populations with greater severity and desolation in many cases, which could be explained by the difficulties that some of these groups have experienced in accessing prevention, diagnosis, and treatment measures, due to lack of information and knowledge, fear associated with their informality or discrimination and marginalization[19],[20].
The untimely experience of the pandemic for international migrant populations in Chile has not necessarily been accompanied by a deep understanding of the degree of knowledge, concerns, and needs felt about COVID-19 by these communities[21],[22]. This is particularly relevant to Venezuelan migrants who have been experiencing social conflict, economic crisis, and poverty for many years before moving to another country, many of them as refugees and asylum seekers[23]. Chile requires a better understanding of how Venezuelan migrants are experiencing and facing the COVID-19 pandemic to promote more equitable and culturally pertinent actions towards preventing and managing this sanitary crisis. To that effect, the following is our research question: “Do Venezuelan migrants in Chile feel prepared to face the pandemic, and what are the variables associated with feeling prepared?” The purpose of this study was to describe the experience of feeling prepared to face the COVID-19 pandemic among Venezuelans residing in Chile.
Methods
Study design
Quantitative observational and cross-sectional study. The study was conducted following a digital opinion poll design.
Procedure
An online self-applied survey was prepared in two languages, Spanish and Creole, aimed at international migrants over 18 who were living in Chile at the time of the survey. The survey included 34 questions and was aimed at identifying, on the one hand, the level of knowledge that immigrant populations in Chile had around COVID-19 and prevention measures and, on the other hand, their immediate needs and concerns towards the future as a consequence of the pandemic. The study design was based on relevant variables from international literature (demographic, socioeconomic, and migration-related variables) and COVID-19 official data from the World Health Organization and the Chilean Ministry of Health (knowledge about its transmission and prevention measures). It was designed with healthcare and migration experts from the participating institutions and piloted with international migrants from different countries of origin (n = 8) before its mass dissemination. The strategy for recruiting and selecting participants in this study was ad-hoc to applying a virtual survey. The survey was shared with various international migrant groups through migrant and pro-migrant organizations and the country’s public health care network. Mailings were made to databases of all the institutions involved, with weekly reinforcement through Facebook, Twitter, email, and WhatsApp standardized messages. Migrant and pro-migrant organizations and groups handed over the invitation to their key contacts following the snowball sampling strategy[24], useful for studies with hard-to-reach populations[25],[26]. Close contact was maintained with these organizations during data collection to ensure, to the maximum extent possible, that the survey was answered by foreign persons effectively during the three weeks that the survey was available for completion (April 4 to 24, 2020).
Participants
The study included adults who reported being international migrants residing in Chile during the COVID-19 pandemic. Those who agreed to participate in the survey confirmed their interest in participating by clicking a digital informed assent before the self-applied survey could be completed. The only exclusion criterion was not having Internet access to answer the survey. After three weeks of dissemination of this survey, an effective sample size of 1 690 participants was reached. This analysis focuses on Venezuelan migrants, who represented 1 008 participants from the general study. All analyses presented in this manuscript were conducted on this subgroup only.
Variables
The main variable was “feeling prepared to face COVID-19” (yes/no). Additional variables were: region of residence in the country, level of education (basic, medium, high), length of stay in Chile (less than six months, six to 12 months, one to five years, five to ten years, more than ten years), type of healthcare provision entitlement (public Fonasa, private Isapre, I don’t know, I don’t have, other), employment status (has a job, doesn’t have but wants to work, does not have and does not want to work), symptoms of anxiety and depression due to the COVID-19 pandemic in the past week (yes/no, respectively), following quarantine (yes/no), feeling well informed about the pandemic (yes/no) and perception of the quality of the information related to COVID-19 provided by government and healthcare teams (very good/good, bad/very bad). Following a survey study design, data were self-reported. Only the questions addressing these variables were taken into account from the survey’s more extensive set of questions.
Data analysis
Missing data was virtually inexistent in this dataset. A descriptive analysis of quantitative and categorical study variables was performed. Proportions and means were estimated for each variable, according to the type of variable. The analysis was conducted for the entire sample first and then stratifying by those reporting feeling prepared versus not feeling prepared to face the COVID-19 pandemic. Data analysis was carried out with Stata 16.
Risk of bias
This was an exploratory, descriptive study. Selection bias due to lack of Internet access by migrants is recognized as a limitation. Other potential selection biases were attempted to be controlled by exhaustive and ample recruitment processes via several relevant institutions that collaborated to disseminate the project and the poll. Information bias was attempted to be controlled by a prior piloting phase of the questionnaire and not including potentially sensitive questions to migrants and a short, simple online format.
Ethical aspects
The opinion poll proposal and questionnaire were revised by a social and ethics committee at collaborative institutions that included international migrants and experts on migration in Chile. Voluntary participation was secured through a digital informed assent from participants, who had to read and confirm their acceptance to participate before starting the survey. No question that could be considered sensitive was included in the survey, such as immigration status, poverty or overcrowding, perceived discrimination, etc. Before its application, the collaborating institutions reviewed the survey, who have experience in opinion polls and work closely with multiple international migrant communities in the country. A secure online software was used, and the database was stored under a password on the principal investigator’s computer. To thank the participants, general information about the rights to health of migrants in Chile at the Digital Observatory on Health of International Migrants of Chile was made available at the online survey’s termination.
Results
The study participants’ average age was 38.1 years (s.d. 10.1), and 71% of the sample was female. Most of the Venezuelan participants in this study had arrived in Chile between one and five years prior (70%) and resided in the Metropolitan Region (69%); 80% achieved a university education; 53% had a job, and 45% did not but wanted to work; 64% were enrolled in the public health system (Fonasa), and 21% indicated that they did not have any health insurance (Table 1).
Table 1. General description of study participants (n = 1008)
78% of Venezuelan participants reported receiving sufficient information about this virus and its disease, but 22% reported that the information was not understandable, and about one in four Venezuelan migrants qualified the information about COVID-19 of poor or very poor quality (23%). 91% reported feeling distressed or worried, and 72% sad or depressed because of the pandemic in the preceding week.
35% of Venezuelan participants reported feeling prepared to face the COVID-19 pandemic, and 65% reported not feeling prepared to face the COVID-19 pandemic. When looking at socio-demographic characteristics of those who reported feeling we prepared, the mean age of this group was 41 (s.d. 10.2) years old, 64% were female, 84% achieved a University education level, 71% had come one to five years ago, and 21% had come six months to a year ago, 55% had a job, and 43% did not have a job but would like to work, 59% belonged to the public healthcare system, and 21% did not have health insurance, and 72% resided in the Metropolitan region. Those who reported not feeling prepared were 37 years old (s.d. 9.6), 75% female, 79% had university-level education, and 20% had a secondary level, 69% had come one to five years ago, and 26% had come six months to a year ago, 53% had a job, and 46% did not have a job but would like to work, 67% belonged to the public healthcare system, and 21% did not have health insurance, and 68% resided in the Metropolitan region (Table 2). That is, compared to Venezuelan migrants who feel prepared to face the COVID-19 pandemic, migrants who reported not feeling prepared were younger and in a higher proportion female, with secondary education level, had arrived in Chile in the past year, do not have a job but want to work, and were covered by the public healthcare provision.
Discussion
The SARS-CoV-2 pandemic hit Chile and the Latin American region with great intensity. It affected the general population, especially older people, those with a history of chronic diseases, people who suffered from excess weight, and some groups experiencing socioeconomic deprivation, including international migrants living in poverty, overcrowding, irregular migratory condition, and informal employment. On March 3, 2020, this virus entered the country through a Chilean traveler who had been vacationing on the Asian continent. Today, the COVID-19 pandemic has spread to the entire national territory and has become a national emergency. Much needs to be done in the coming months to support the health of the Chilean and migrant population residing in the country, as the pandemic’s negative consequences are still to be known.
This study shows that Venezuelan migrants in Chile present low levels of preparedness with regards to the sanitary crisis, as only 35% of respondents reported feeling prepared. Receiving good quality information about the pandemic and how Venezuelan migrants deal with mental health symptoms like anxiety and depressive symptoms are important factors for feeling prepared to face COVID-19 in Chile. Both dimensions are potentially modifiable to influence better health care for migrants in times of pandemic. These results are consistent with what is being presented by international evidence in the context of the international migrant population’s situation facing the COVID-19 pandemic.
Our findings suggest that increased attention towards the health of Venezuelan migrants in Chile and the region is needed. The data documenting how Venezuelan migrants are coping with the COVID-19 crisis is scarce, yet available evidence suggests that they are struggling[23]. Reinforcing measures to support Venezuelan migrants during and after this sanitary crisis has been recommended[27],[28]. Actions related to protecting their health and healthcare are urgent and should be based upon the pillars and principles of public health, human rights, solidarity, and equity. Further actions towards universal health coverage and a transnational approach to continuity of care are needed. As the Venezuelan exodus has proven in recent years, the regional health care agenda should leave no one behind. Structural inequalities and deficiencies of healthcare systems in many Latin American countries quickly reappear when massive movements of people within the region and sanitary crises take place. Discriminatory and xenophobic situations tend to increase, as countries and healthcare systems are tensioned and exhausted by their incapacity to provide solutions when they are needed. The COVID-19 pandemic is a huge stressor, but it can also become an opportunity for creating and implementing novel strategies to deliver and maintain health care in our region, in which regional cooperation might be a large part of the answer.
There is consensus that the COVID-19 pandemic is exacerbating the precarious situation of migrant populations globally and Venezuelan migrants regionally[29]. Some authors even indicate that ongoing global efforts to support international migrant groups in the wake of the pandemic have failed in their task[27],[28]. Prevention measures aimed at international migrants, regardless of their immigration status, age, country of origin, or employment status, has been outlined as a priority issue for global public health[21],[29]. This is of great relevance given the barriers that have been identified worldwide for the access and use of healthcare by the migrant population during the COVID-19 pandemic and the measures promoted by health authorities at the global level. Additionally, the evidence accounts for a general lack of information regarding COVID-19 in the migrant population globally[29],[30],[31],[32]. Furthermore, for some migrant groups, most countries’ social distancing and hygiene improvement measures are challenging to comply with[19].
The general scientific literature on the field has documented that migrant populations present worse health results than the national population in various areas, including mental health. Under non-pandemic conditions, the international migrant population generally presents higher rates of common mental health disorders such as depression and a lower quality of life than the local population[33]. These health issues are being exacerbated during the current COVID-19 crisis[20]. In that sense, there is a need to ensure that migrant populations can access physical and mental healthcare and information relevant and culturally sensitive[29],[31]. Little is known in the Latin American region about how Venezuelan migrants are experiencing and coping with the COVID-19 pandemic. This study aims to provide novel descriptive evidence on this subject, as the Venezuelan exodus to countries in the Latin American region continues to raise challenges and pitfalls.
The study presents some limitations. First, this is a descriptive and cross-sectional study based on an opinion poll that does not allow any causal interpretation. Second, the online application of the questionnaire allowed a broad scope in a short amount of time but did not allow us to add more sensitive questions. Hence, this study is only exploratory and should be improved through more detailed quantitative and qualitative studies in the future. However, to the best of our knowledge, this is the first study in Venezuelan migrant populations dedicated to describing how they face the SARS-CoV-2 pandemic. We hope that future studies will delve into these general results and that, despite its limitations, study findings will be considered for decision-making regarding the Venezuelan population in Chile and the region, regarding the issues of access, protection, and prevention in health, both during the current health crisis and future ones.
We conclude that Venezuelan migrants in Chile present low levels of preparedness regarding the sanitary crisis, as only 35% of respondents reported feeling prepared. Receiving good quality information about the pandemic and how Venezuelan migrants deal with mental health symptoms like anxiety and depressive symptoms are important factors for feeling prepared to face COVID-19 in Chile. These elements need further attention in Chile in the management of the present pandemic and the preparedness and response of future ones.
Notes
Authorship contributions
BC: Conceptualization, data curation, funding acquisition, methodology, project administration, supervision, validation, writing original draft. FD: Data curation, formal analysis, software, validation, writing original draft. AB: Conceptualization, methodology, resources, project administration, validation, writing original draft. AO: Conceptualization, funding acquisition, project administration, supervision, validation, writing original draft. CS: Methodology, supervision, validation, writing original draft.
Competing interests
Each author declares there are no competing interests with the content of this article.
Funding
National Fund for Health Research and Development SA19I0066, National Agency of Research and Development(ex-National Commission for Scientific and Technological Research), Chilean Government.
National Agency of Research and Development Millennium Science Initiative/ Millennium Initiative for Collaborative Research on Bacterial Resistance, MICROB-R, NCN17_081.
Supplementary files
None.
Acknowledgments
We appreciate the support of the following: Nkulama Saint Louis, José Tomás Vicuña, Matías Libuy, José Manuel Munita, Alejandra Carreño, and Carla Urrutia. We acknowledge and appreciate the collaboration of all the international migrants who answered this survey, as well as the institutions and people who supported this study: Jesuit Migrant Service, Migration and Health Commission at the Medical College of Chile, Millennium Nucleus of Antimicrobial Resistance MICROB-R, Interdisciplinary Research Network on Infectious Diseases, Catholic Institute for Migration, Seremi de Salud de la Región Metropolitana, Healthcare Network at the national level, Undersecretary of Healthcare Networks of the Ministry of Health through its International Migrants Reference, Mr. Daniel Molina, Collectives and organizations of international migrants, Community leaders and managers, ChileCientífico, Referents of migrants from the assistance network.

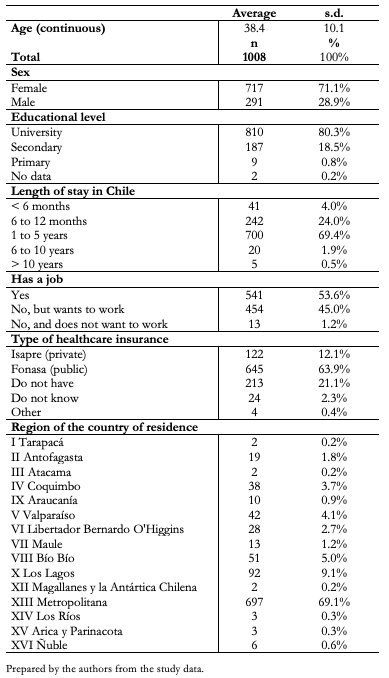 Table 1. General description of study participants (n = 1008)
Table 1. General description of study participants (n = 1008)
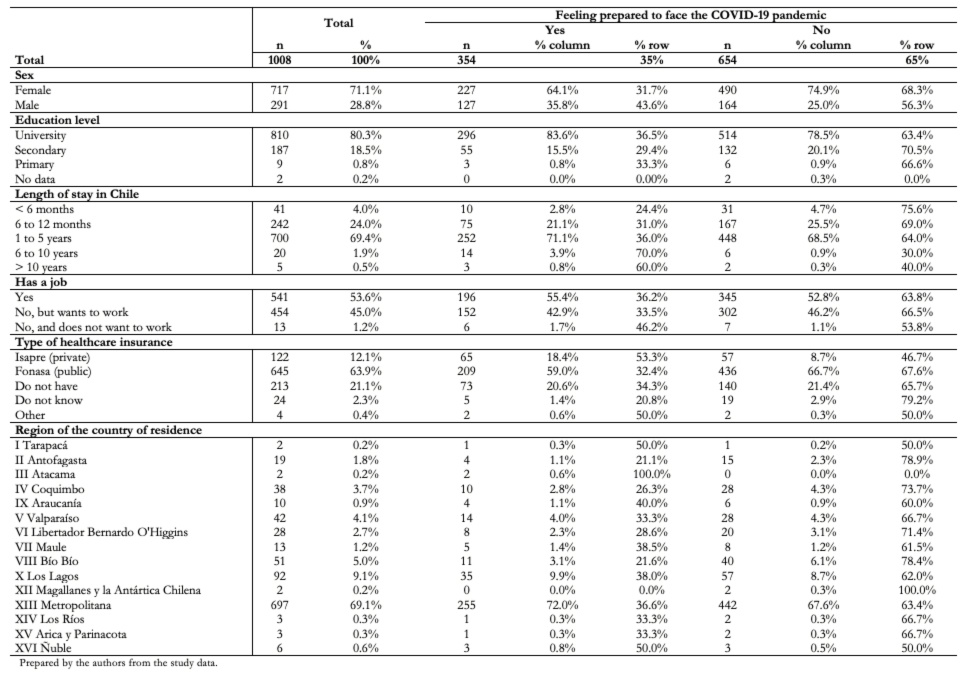 Table 2. Socio-demographic characteristics of study participants according to feeling prepared/ not feeling prepared to face the COVID-19 pandemic among Venezuelan migrants in Chile (n = 1008)
Table 2. Socio-demographic characteristics of study participants according to feeling prepared/ not feeling prepared to face the COVID-19 pandemic among Venezuelan migrants in Chile (n = 1008)
 Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
Esta obra de Medwave está bajo una licencia Creative Commons Atribución-NoComercial 3.0 Unported. Esta licencia permite el uso, distribución y reproducción del artículo en cualquier medio, siempre y cuando se otorgue el crédito correspondiente al autor del artículo y al medio en que se publica, en este caso, Medwave.
Introducción
La migración internacional es un determinante social de la salud que puede influir en los resultados de salud de un individuo y su comunidad. La última década ha experimentado un gran éxodo desde Venezuela a otros países de la región, incluido Chile. En los últimos meses, el mundo se ha enfrentado a la pandemia de coronavirus del SARS-CoV-2 y su enfermedad respiratoria COVID-19.
Objetivo
Explorar qué factores están asociados con sentirse preparado para enfrentar la pandemia de COVID-19 entre la población venezolana que reside en Chile.
Métodos
Estudio cuantitativo transversal, siguiendo el diseńo de una encuesta de opinión. Encuesta auto-aplicada en línea en espańol y Creol haitiano, que fue diseńada y puesta a prueba con expertos y migrantes internacionales. Se difundió a varios grupos internacionales de migrantes a través de redes de organizaciones de migrantes y pro-migrantes, así como a través de la red chilena de atención de salud pública en todo el territorio nacional. Tamańo de muestra de 1690 participantes, de los cuales 1008 (60%) eran de Venezuela y se incluyeron en este análisis descriptivo. Se analizó en forma descriptiva la variable principal sentirse preparado para enfrentar la pandemia de COVID-19 (sí/no) así como las variables sexo, nivel educacional, tiempo de estadía en Chile, tipo de previsión de salud, ansiedad o depresión debido a COVID-19, cumplimiento de confinamiento y evaluación de calidad de la información sobre COVID-19 que se ha recibido de autoridades y equipos de salud.
Resultados
65% de los participantes venezolanos informaron no sentirse preparados para la pandemia. En comparación con los migrantes venezolanos que se sienten preparados para enfrentar la pandemia de COVID-19, los migrantes venezolanos que reportaron no sentirse preparados eran en mayor proporción mujeres, con nivel de educación secundaria, habían llegado a Chile en el último ańo, no tienen trabajo pero quieren trabajar, y pertenecer a la prestación sanitaria pública.
Discusión
Recibir información de buena calidad sobre la pandemia y la salud mental son factores importantes asociados con sentirse preparado para enfrentar COVID-19 en migrantes venezolanos en Chile, lo cual sugiere que se necesita más atención en la salud física y mental de los migrantes venezolanos en Chile y en la región.
Authors:
Báltica Cabieses[1], Florencia Darrigrandi[2], Alice Blukacz[1], Alexandra Obach[1], Claudia Silva[1]
Affiliation:
[1] Programa de Estudios Sociales en Salud, Instituto de Ciencias e Innovación en Medicina (ICIM), Facultad de Medicina Clínica Alemana, Universidad del Desarrollo, Santiago, Chile
[2] Facultad de Ingeniería y Ciencias, Universidad Adolfo Ibáńez, Santiago, Chile
E-mail: bcabieses@udd.cl
Author address:
[1] Avenida Las Condes 12.461, Las Condes
Santiago, Chile
Citation: Cabieses B, Darrigrandi F, Blukacz A, Obach A, Silva C. Feeling prepared to face COVID-19 pandemic among Venezuelans in Chile: findings from an opinion poll. Medwave 2021;21(01):e8103 doi: 10.5867/medwave.2021.01.8103
Submission date: 18/8/2020
Acceptance date: 10/11/2020
Publication date: 8/2/2021
Origin: Not commissioned.
Type of review: Externally peer-reviewed by three reviewers, double-blind.
Comments (0)
We are pleased to have your comment on one of our articles. Your comment will be published as soon as it is posted. However, Medwave reserves the right to remove it later if the editors consider your comment to be: offensive in some sense, irrelevant, trivial, contains grammatical mistakes, contains political harangues, appears to be advertising, contains data from a particular person or suggests the need for changes in practice in terms of diagnostic, preventive or therapeutic interventions, if that evidence has not previously been published in a peer-reviewed journal.
No comments on this article.
To comment please log in
Medwave provides HTML and PDF download counts as well as other harvested interaction metrics. There may be a 48-hour delay for most recent metrics to be posted.
- Segal UA. Globalization, migration, and ethnicity. Public Health. 2019 Jul;172:135-142. | CrossRef | PubMed |
- International Organization for Migration. Glossary on Migration. Geneva. 2019. [Internet] | Link |
- Wingens M, Windzio M, Valk H de, Aybek C. A Life-Course Perspective on Migration and Integration. Springer Netherlands 2011. | CrossRef |
- Castańeda H, Holmes SM, Madrigal DS, Young ME, Beyeler N, Quesada J. Immigration as a social determinant of health. Annu Rev Public Health. 2015 Mar 18;36:375-92. | CrossRef | PubMed |
- Davies A, Basten A, Frattini C. Migration: A Social Determinant of the Health of Migrants. Eurohealth 2010;16:10–2. [Internet] | Link |
- Espinoza M, Rodríguez C, Cabieses B. Manual para la participacion de pacientes en toma de decisiones sobre cobertura en salud. Santiago, Chile. Pontificia Universidad Católica de Chile. 2019.
- Cabieses B. Salud y migración: un proceso complejo y multidimensional. In: Migración en Chile: Evidencia y mitos de una nueva realidad. Santiago: LOM 2019. 143–70.
- Thomas F. Handbook of Migration and Health. Edward Elgar Publishing 2016.
- Cabieses B, Chepo M, Oyarte M, Markkula N, Bustos P, Pedrero V, et al. [Health inequality gap in inmigrant versus local children in Chile]. Rev Chil Pediatr. 2017 Dec;88(6):707-716. | CrossRef | PubMed |
- Cabieses B, Oyarte M. Health access to immigrants: identifying gaps for social protection in health. Rev Saude Publica. 2020 Feb 17;54:20. | CrossRef | PubMed |
- Markkula N, Cabieses B, Lehti V, Uphoff E, Astorga S, Stutzin F. Use of health services among international migrant children - a systematic review. Global Health. 2018 May 16;14(1):52. | CrossRef | PubMed |
- Hagen-Zanker J, Mosler Vidal E, Sturge G. Social protection, migration and the 2030 Agenda for Sustainable Development. Swiss Agency for Development and Cooperation 2017. [Internet] | Link |
- Velásquez Pinto M, Yáńez Betancourt L, Molina Castro F. Inserción laboral de los trabajadores migrantes en el sector rural en Chile. Santiago: OIT 2020. [Internet] | Link |
- UNESCO, UN-HABITAT. Migrants’ Inclusion in Cities: Innovative Urban Policies and Practices. 2012. [Internet] | Link |
- Riggirozzi P, Grugel J, Cintra N. Protecting Migrants or Reversing Migration? COVID-19 and the risks of a protracted crisis in Latin America. 2020. [internet] | Link |
- United Nations Network on Migration. COVID-19 does not discriminate, nor should our response. (accessed June 29 2020). [Internet] | Link |
- Estadísticas Migratorias. Dep. Extranj. Migr. (accessed April 21 2020). [Internet] | Link |
- COVID-19 Map. Johns Hopkins Coronavirus Resour. Cent. (accessed August 4 2020). [Internet]. | Link |
- Orcutt M, Patel P, Burns R, Hiam L, Aldridge R, Devakumar D, et al. Global call to action for inclusion of migrants and refugees in the COVID-19 response. Lancet. 2020 May 9;395(10235):1482-1483. | CrossRef | PubMed |
- Orcutt M, Spiegel P, Kumar B, Abubakar I, Clark J, Horton R; Lancet Migration. Lancet Migration: global collaboration to advance migration health. Lancet. 2020 Feb 1;395(10221):317-319. | CrossRef | PubMed |
- Page KR, Venkataramani M, Beyrer C, Polk S. Undocumented U.S. Immigrants and Covid-19. N Engl J Med. 2020 May 21;382(21):e62. | CrossRef | PubMed |
- Mesa Vieira C, Franco OH, Gómez Restrepo C, Abel T. COVID-19: The forgotten priorities of the pandemic. Maturitas. 2020 Jun;136:38-41. | CrossRef | PubMed |
- Daniels JP. Venezuelan migrants "struggling to survive" amid COVID-19. Lancet. 2020 Mar 28;395(10229):1023. | CrossRef | PubMed |
- Sadler GR, Lee HC, Lim RS, Fullerton J. Recruitment of hard-to-reach population subgroups via adaptations of the snowball sampling strategy. Nurs Health Sci. 2010 Sep 1;12(3):369-74. | CrossRef | PubMed |
- Aglipay M, Wylie JL, Jolly AM. Health research among hard-to-reach people: six degrees of sampling. CMAJ. 2015 Oct 20;187(15):1145-1149. | CrossRef | PubMed |
- Faugier J, Sargeant M. Sampling hard to reach populations. J Adv Nurs. 1997 Oct;26(4):790-7. | CrossRef | PubMed |
- Espinel Z, Chaskel R, Berg RC, Florez HJ, Gaviria SL, Bernal O, et al. Venezuelan migrants in Colombia: COVID-19 and mental health. Lancet Psychiatry. 2020 Aug;7(8):653-655. | CrossRef | PubMed |
- Figueira J, Zaim SR. How a team of Venezuelan expats is fighting COVID-19 at home. Nature. 2020 Jun 12. | CrossRef | PubMed |
- Kluge HHP, Jakab Z, Bartovic J, D'Anna V, Severoni S. Refugee and migrant health in the COVID-19 response. Lancet. 2020 Apr 18;395(10232):1237-1239. | CrossRef | PubMed |
- Liem A, Wang C, Wariyanti Y, Latkin CA, Hall BJ. The neglected health of international migrant workers in the COVID-19 epidemic. Lancet Psychiatry. 2020 Apr;7(4):e20. | CrossRef | PubMed |
- Fernández-Nińo JA, Cubillos-Novella A, Bojórquez I, Rodríguez M. Recommendations for the response against COVID-19 in migratory contexts under a closed border: The case of Colombia. Biomedica. 2020 Oct 30;40(Supl. 2):68-72. | CrossRef | PubMed |
- Joob B, Wiwanitkit V. COVID-19 and migrant workers: Lack of data and need for specific management. Public Health. 2020 Jun;183:64. | CrossRef | PubMed |
- Foo SQ, Tam WW, Ho CS, Tran BX, Nguyen LH, McIntyre RS, et al. Prevalence of Depression among Migrants: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2018 Sep 12;15(9):1986. | CrossRef | PubMed |
Segal UA. Globalization, migration, and ethnicity. Public Health. 2019 Jul;172:135-142. | CrossRef | PubMed |Wingens M, Windzio M, Valk H de, Aybek C. A Life-Course Perspective on Migration and Integration. Springer Netherlands 2011. | CrossRef |Castańeda H, Holmes SM, Madrigal DS, Young ME, Beyeler N, Quesada J. Immigration as a social determinant of health. Annu Rev Public Health. 2015 Mar 18;36:375-92. | CrossRef | PubMed |Davies A, Basten A, Frattini C. Migration: A Social Determinant of the Health of Migrants. Eurohealth 2010;16:10–2. [Internet] | Link |Espinoza M, Rodríguez C, Cabieses B. Manual para la participacion de pacientes en toma de decisiones sobre cobertura en salud. Santiago, Chile. Pontificia Universidad Católica de Chile. 2019. Cabieses B. Salud y migración: un proceso complejo y multidimensional. In: Migración en Chile: Evidencia y mitos de una nueva realidad. Santiago: LOM 2019. 143–70. Thomas F. Handbook of Migration and Health. Edward Elgar Publishing 2016. Cabieses B, Chepo M, Oyarte M, Markkula N, Bustos P, Pedrero V, et al. [Health inequality gap in inmigrant versus local children in Chile]. Rev Chil Pediatr. 2017 Dec;88(6):707-716. | CrossRef | PubMed |Cabieses B, Oyarte M. Health access to immigrants: identifying gaps for social protection in health. Rev Saude Publica. 2020 Feb 17;54:20. | CrossRef | PubMed |Markkula N, Cabieses B, Lehti V, Uphoff E, Astorga S, Stutzin F. Use of health services among international migrant children - a systematic review. Global Health. 2018 May 16;14(1):52. | CrossRef | PubMed |Hagen-Zanker J, Mosler Vidal E, Sturge G. Social protection, migration and the 2030 Agenda for Sustainable Development. Swiss Agency for Development and Cooperation 2017. [Internet] | Link |Velásquez Pinto M, Yáńez Betancourt L, Molina Castro F. Inserción laboral de los trabajadores migrantes en el sector rural en Chile. Santiago: OIT 2020. [Internet] | Link |UNESCO, UN-HABITAT. Migrants’ Inclusion in Cities: Innovative Urban Policies and Practices. 2012. [Internet] | Link |Riggirozzi P, Grugel J, Cintra N. Protecting Migrants or Reversing Migration? COVID-19 and the risks of a protracted crisis in Latin America. 2020. [internet] | Link |United Nations Network on Migration. COVID-19 does not discriminate, nor should our response. (accessed June 29 2020). [Internet] | Link |COVID-19 Map. Johns Hopkins Coronavirus Resour. Cent. (accessed August 4 2020). [Internet]. | Link |Orcutt M, Patel P, Burns R, Hiam L, Aldridge R, Devakumar D, et al. Global call to action for inclusion of migrants and refugees in
the COVID-19 response. Lancet. 2020 May 9;395(10235):1482-1483. | CrossRef | PubMed |Orcutt M, Spiegel P, Kumar B, Abubakar I, Clark J, Horton R; Lancet
Migration. Lancet Migration: global collaboration to advance migration health.
Lancet. 2020 Feb 1;395(10221):317-319. | CrossRef | PubMed |Page KR, Venkataramani M, Beyrer C, Polk S. Undocumented U.S. Immigrants and
Covid-19. N Engl J Med. 2020 May 21;382(21):e62. | CrossRef | PubMed |Mesa Vieira C, Franco OH, Gómez Restrepo C, Abel T. COVID-19: The forgotten
priorities of the pandemic. Maturitas. 2020 Jun;136:38-41. | CrossRef | PubMed |Daniels JP. Venezuelan migrants "struggling to survive" amid COVID-19.
Lancet. 2020 Mar 28;395(10229):1023. | CrossRef | PubMed |Sadler GR, Lee HC, Lim RS, Fullerton J. Recruitment of hard-to-reach
population subgroups via adaptations of the snowball sampling strategy. Nurs
Health Sci. 2010 Sep 1;12(3):369-74. | CrossRef | PubMed |Aglipay M, Wylie JL, Jolly AM. Health research among hard-to-reach people:
six degrees of sampling. CMAJ. 2015 Oct 20;187(15):1145-1149. | CrossRef | PubMed |Faugier J, Sargeant M. Sampling hard to reach populations. J Adv Nurs. 1997
Oct;26(4):790-7. | CrossRef | PubMed |Espinel Z, Chaskel R, Berg RC, Florez HJ, Gaviria SL, Bernal O, et al. Venezuelan migrants in Colombia: COVID-19 and mental
health. Lancet Psychiatry. 2020 Aug;7(8):653-655. | CrossRef | PubMed |Figueira J, Zaim SR. How a team of Venezuelan expats is fighting COVID-19 at
home. Nature. 2020 Jun 12. | CrossRef | PubMed |Kluge HHP, Jakab Z, Bartovic J, D'Anna V, Severoni S. Refugee and migrant
health in the COVID-19 response. Lancet. 2020 Apr 18;395(10232):1237-1239. | CrossRef | PubMed |Liem A, Wang C, Wariyanti Y, Latkin CA, Hall BJ. The neglected health of
international migrant workers in the COVID-19 epidemic. Lancet Psychiatry. 2020
Apr;7(4):e20. | CrossRef | PubMed |Fernández-Nińo JA, Cubillos-Novella A, Bojórquez I, Rodríguez M.
Recommendations for the response against COVID-19 in migratory contexts under a
closed border: The case of Colombia. Biomedica. 2020 Oct 30;40(Supl. 2):68-72. | CrossRef | PubMed |





 Research papers
Research papersSystematization of initiatives in sexual and reproductive health about good practices criteria in response to the COVID-19 pandemic in primary health care in Chile
Clinical, psychological, social, and family characterization of suicidal behavior in Chilean adolescents: a multiple correspondence analysis
